Coordinating the safe and timely travel of 2 physicians, 2 paramedics/RNs and 1 Rotarian from 2 different states and 3 different cities is no small undertaking. In addition to personnel, we had the added challenge of getting 300+ pounds worth of medical training equipment including CPR mannequins, needle decompression trainers and oxygen bottles to Rwanda with us. We found out about 4 weeks before we were to fly that these things aren’t readily available for purchase where we are headed.
We are going to Kigali, the capital of Rwanda, to teach. Our mission is to help build and solidify a formal EMS system with top-notch Prehospital trauma care. Ambulances in Kigali are currently operated by SAMU, but the providers are nurses rather than Paramedics or EMTs. That’s because there are no formal EMS certifications or programs there. Our aim is to provide the current workforce with prehospital-specific trauma training to improve provider safety. 50% of all EMS calls in Kigali are for motor vehicle collisions (MVCs). MVC trauma is a major cause of morbidity and mortality across Rwanda.
We carpooled from Richmond to Dulles. Basil, the creator of the Trauma Course content, was kind enough to offer up his Ford Explorer. More challenging than the traffic on I-95 though, were the back seat drivers offering our opinions on the best route. Dr. Sudha, a Trauma Surgeon and myself, an Emergency Physician – we are accustomed to being the pilots.
Fortunately the traffic gods showed us mercy, and we arrived at Dulles slightly ahead of schedule. The next challenge – get the 300+ lbs of luggage and equipment from the Explorer into the international terminal. It didn’t take long for the bellcap to notice me struggling to hoist a gigantic red backpack onto my back while desperately reaching for my rollerbag that was attempting to escape into traffic. He hurried towards us with his cart and began stacking our ridiculous assemblage of oversized bags. I can only imagine what he thought of us – between the bags marked “adult/child/infant” and “torso,” he must have thought we were body smugglers or really bad parents.
Inside the terminal, he unloaded our bags. I reached for some cash, knowing I was one of the few of us with smaller bills. In our pre-trip prep, Sudha advised us ahead of time to get $100 bills from the bank. In Rwanda, the larger the bill, the higher the exchange rate. I handed him the money and was met with a confused look. “Not enough, I said?” feeling confused and bordering on embarrassed. He mumbled something unintelligible but his face told me it wasn’t good. Frank, the Rotarian accompanying us on the trip, quickly slipped him more cash, which seemed to placate him as he then scurried away.
I have Dr. Sudha to thank for the opportunity to be on this trip. She’s a fellowship trained Trauma Surgeon with a focus on International Medicine. She and I have worked together for over three years in the Emergency Department at VCU taking care of trauma patients who suffer accidents and injuries throughout Central Virginia. She first travelled to Rwanda 7 years ago during her fellowship and has since made over 20 separate trips. (I get the sense she just stopped counting at some point). In October 2017, she was awarded 3 grants totaling over $700,000, one of which was from Rotary International; hence Frank’s presence with us on the trip. If you know her, you understand why she was trusted with so much money. She’s just impressive.
The 5th person travelling with us is Jane. A nurse and a volunteer paramedic in Deltaville, VA, Jane worked at VCU for years in multiple capacities. Over time, she’s carved out a niche in International EMS, so she was an obvious choice for the team.
Frank, Jane, Stephanie, Sudha and Basil
At the KLM* counter, we were met with friendliness and curiosity regarding our absurd quantity of baggage. We opted to check the medical equipment and carry-on our personal belongings. We didn’t want to take a gamble on the reliability of baggage transfer from Amsterdam to Kigali and end up with endotracheal tubes but no underwear.
I’ve decided for the privacy of those with me on the trip that I won’t include them from here on out. After all, this is just my perspective, and I don’t want to give the false appearance that I speak for anyone else. I will say I’m with a unique group of people and look forward to getting to know these like-minded folks. At dinner Dr. Sudha asked if we’d rather spend our 2 days off on a safari or at museums. The reflexive and immediate consensus was “SAFARI!” I knew then this was going to be a great trip.
*Bonus points for the free drinks on KLM.
Jan 21, 2018
“Day 2” is a bit of a misnomer. Technically it’s the 21st, but only because we just jumped ahead 6 hours by time zone. That didn’t stop KLM from feeding us breakfast just 1.5 hours after we’d eaten a full dinner.
We landed in Amsterdam without a hiccup. The last time I was in this airport was December of 2002. I’d just spent 5 months living in Spain, taking advanced conversational Spanish classes. What I didn’t realize then was just what a turn my life would take. I’d gone to Spain for a reset. I’d hit some professional hiccups in my last job and went to Spain, I thought, to do the study abroad I never had the chance to do while at UVA. Yes, I became fluent in Spanish, but I also found myself and my way forward.
What’s amazing about your twenties is the same thing that makes that time very lonely. You’ve left the nest, launched into a wide-open world full of opportunity, choices and possibilities. But you’ve left your nuclear family. And unlike decades prior, your independence isn’t quickly followed by love, marriage and establishment of your own nuclear family. There’s a gap now, a road with thousands of potential turns, each of which could lead to an entirely different life. Endless opportunity can be paralyzing. After standing at that airport, I came home, applied for and landed a job, which resulted in a successful career in Internet Marketing. I also joined my local rescue squad.
The view from the window on this leg of our journey, Amsterdam to Kigali, can be summed up in one word: tan. I finally gave in to my body’s repeated requests and took a 2 hour nap. Since waking up, I’ve seen nothing but desert. I did have a view of a beautiful part of Africa on the plane itself. Wearing a handmade, yellow and green gown with her hair secured tightly in a bright yellow wrap, everyone’s eyes focused on this woman when she appeared at the boarding gate. I looked down at my hold-over maternity pants and Merrill shoes and suddenly felt boorish and underdressed.
We arrived on time into Kigali. I had hoped for daylight as we landed so I could take an aerial survey of the city, but this close to the equator, night overcomes day very quickly, with sunsets happening in about 10 minutes from daylight to darkness.
We’re staying at the Gloria Hotel , which is just the right combination of nice but not stuffy. My only regret again is that it’s dark, and I can’t fully appreciate everything the area has to offer. I’m settling into my room as we have a long day tomorrow spending time in the Emergency Department, on the SAMU ambulance, and hopefully paying our respects at the Genocide Museum
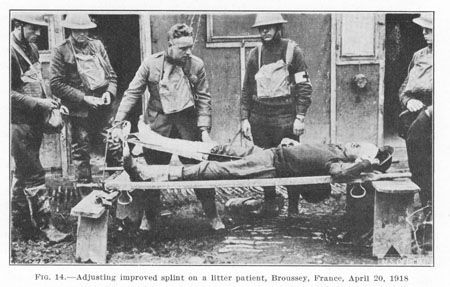
Traction splints have been around since the late 1800s and were first employed during WWI. Given the lack of alternatives and atrocious environment, they were credited with massively lowering the mortality rate of soldiers suffering femur fractures on the battlefield. The idea was simple – take the long, sharp shards of broken bone, which exist within millimeters of the largest artery in the body, and stabilize them to ease pain and help control or prevent massive bleeding.
A century later, little has changed. There are a few basic flavors, but all have the essentially the same design of a long rod that runs against the affected leg and something which with to pull tension upon and secure the foot or ankle. Despite a lack of continued innovation and even less in the way of empiric research, an almost identical device to that which made its debut with the British Army in 1915 is required aboard every ground ambulance in the country. And almost every one of them resides in a cabinet or under a bench, forgotten and ignored until the biennial state inspection rolls around.
The “Thomas Splint,” c. 1915
All EMTs are taught the procedure for applying a traction splint, but too often it is done in the classroom then never again. In my own experience of almost a decade of EMS, I have had the opportunity to apply one only once. As an ER physician for the last three years at the largest, busiest trauma center in Virginia, I have yet to have a patient arrive with one in place. My theory is that providers often do not consider it when appropriate, and even when they do their familiarity and comfort with the procedure is lacking, so it is skipped. In fact, one study found them to be applied in only 38% of appropriate cases and of those, 2/3 were placed incorrectly.
In other words, if you happen to break your leg, there is only about a 13% chance someone will correctly stabilize that razor sharp bone jostling against your femoral artery while you bump along to the hospital.
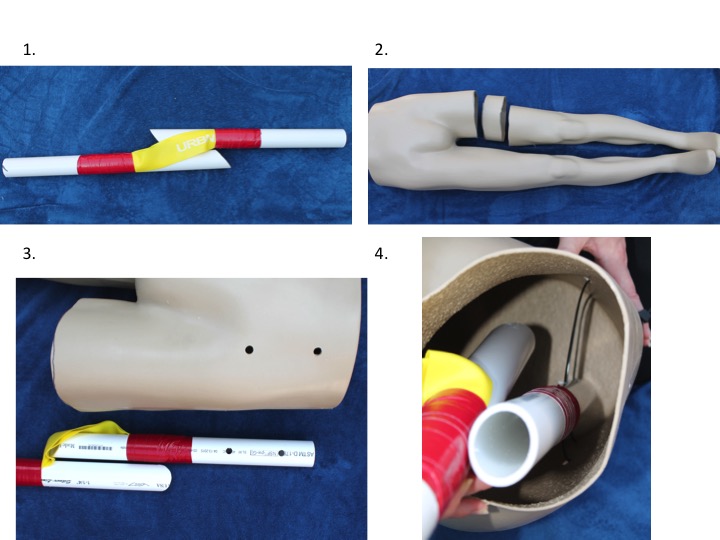
Since accurately practicing the procedure without crippling and otherwise healthy recruit is difficult, I looked up available traction splint training models. They cost around $1800, and are full of unnecessary bells and whistles, well beyond the means of many small EMS agencies. So I took matters into my own hands and created a rugged, reliable, anatomically and physiologically accurate model for less than $75. I’m offering it here, open sourced, to anyone who may want to replicate it for his or her training department.
Rubber exercise bands were stretched along the length of a two foot long section of 1 ½” PVC pipe, using duct tape to secure either end. The pipe was then cut diagonally in the middle, simulating a fractured bone.
A six-inch section of the mannequin’s thigh was removed.
Matching holes were drilled in the proximal and distal sections of the “broken femur” and the mannequin leg.
The simulated bone was inserted and secured at both ends with long zip ties passed through the holes.
At rest, the proximal and distal segments of the mannequin leg fit together, accurately simulating the shortened extremity one would expect with such an injury. The exercise bands create a physiologic level of tension, and the leg can be pulled to length and stabilized using any commercially available traction splint. At length, the gap created allows the learner to visualize the physiology of the injury and intended function of the device.
If you do make one, please post a comment and let us know how it turned out!
American College of Surgeons (2009). Equipment for Ambulances. https://www.facs.org/~/media/files/qualityprograms/trauma/publications/ambulance.ashx
American College of Surgeons (2012). Chapter 8 Musculoskeletal Trauma. Advanced Trauma Life Support Student Manual. 219-220
Abarbanell, N. (2001) Prehospital Midthigh Trauma and Traction Splint Use: Recommendations for Treatment Protocols. American Journal of Emergency Medicine. 19 (2). 137-140.
Skelton MB and NE McSwain (1997). A Study of Cognitive and Technical Skill Deterioration Among Trained Paramedics. Journal of the American College of Emergency Physicians. 6 (10). 436-438.
Daughtery, M., Mehlman, C., Moody, S., LeMaster, T., & Falcone, R. (2013) Significant Rate of Misuse of the Hare Traction Splint for Children with Femoral Shaft Fractures. Journal of Emergency Nursing. 39. 97-103.
I put this video together last year for my parent’s 50th Wedding Anniversary. I’m moving it here for hosting as YouTube took it down a few weeks ago citing copyright concerns. I guess my 212 views were a threat.
One of the things I’ve most looked forward to since Steph and I toured all over the country interviewing at 20+ residency programs was the prospect of an “elective” month. Almost every program had a month carved out for residents to choose an area of (educational) interest and immerse themselves however they pleased. Finally, after three years of waiting, this year was my chance.
I researched for months and finally settled on traveling to London to work with and learn from the London Ambulance Service, one of the world’s premier prehospital agencies. Combined with the emergency physicians aboard the London Air Ambulance, they are doing some cutting edge stuff – including point of care ultrasound, field thoracotomies, REBOA and true prehospital critical care. Plus I’d have a chance to visit Grandma.
So, needless to say, I was bummed when the opportunity failed to materialize.
But as luck would have it, just a few days later I bumped into Dr. Ornato, the chairman of our department at VCU. I mentioned it to him, and without skipping a beat he asked, “Want to go to Singapore?”
Fun Fact #1: Singapore is a tiny island city-state, meaning the entire country is one big city (think Ancient Greece, but Asian). It has been at the center of the global economy for hundreds of years, from a refueling port for the British East India Company to what is now one of the largest shipping ports in the world, with up to 100,000 vessels traversing the Strait of Singapore yearly.
Now when I say Singapore is far away, consider this: the Earth is roughly 24,000 miles around and this was a 12,000 mile flight. If I’d have gone any further I’d have been on my way back home. (And did I mention I was in a middle seat? My knees, back and bladder were not amused. But I digress.) Roughly two days after setting off I landed as far from home as I’d ever been and will likely ever be (until I make it into orbit, that is).
My first impression both in the airport moving through customs and in the taxi on the way to the place where I’d be stay for the next ten days was pleasant surprise at just how clean, efficient and organized the whole place seemed to be. No pushing or even a raised voice, just well designed infrastructure ready to welcome visitors, students, investors and most importantly: me.
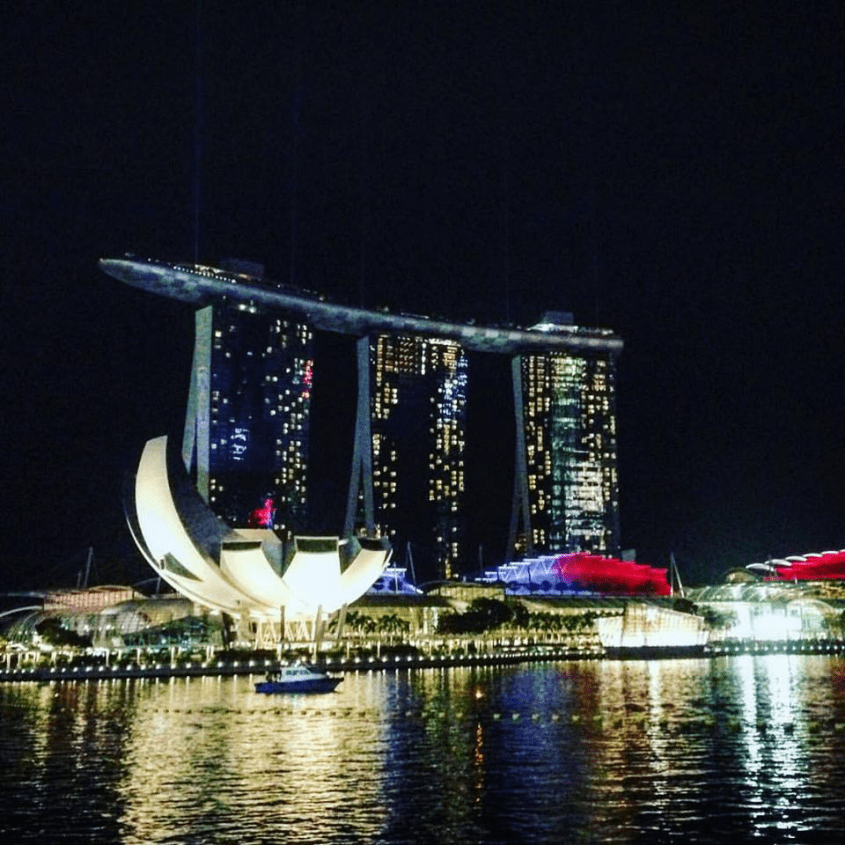
Marina Bay Sands with the Art-Science Museum on the left
I decided to try AirBnb for the first time. I was traveling alone and found it to be much cheaper than hotels, so why not give it a shot. There was of course the possibility of being murdered in a stranger’s home, and every listing looked far too good to be true, but hell what’s life without a little risk of being drugged and dismembered in your sleep every now and then. So I settled on a condo in an upscale residential district which boasted four swimming pools, a hot tub, free wifi, private bedroom and bathroom, plus walking distance to two subway stations, restaurants, shopping, and a few of Singapore’s ubiquitous dining halls (more on that later), all for less than $60/night. See what I mean?! Must be too good to be true.
But it wasn’t! I found the apartment to be exceptionally comfortable and convenient, precisely as advertised. I met my hosts – an American/Chinese Harvard grad and a Moroccan/French banker – who didn’t seem like serial killers at all. Again, pleasantly surprised and more than a little relieved.
I arrived early and had slept for 16 hours all the way across the Pacific, so after getting settled I was ready to explore. I stepped outside to an instant reminder that the country lies just one degree north of the Equator – instant, drenching perspiration. Nevertheless, I spent the first two days exploring the tiny country on foot, sweating profusely.
Gardens by the Bay
Singapore is about half the size of London or Los Angeles with a population of just over five million. One of the most striking things about it was the diversity – a nation made up of Chinese, Indian, Malay, European and dozens of other nationalities living in near-complete harmony. That, combined with an effective, non-corrupt government, has attracted tremendous investment, and in just one generation the little city-state has blossomed to become a global center of commerce, ranking 7th in GDP per capita world-wide.
Hand carved decorations at the Sri Veeramakaliamman Temple in Little India. Next door were two Buddhist temples.
Fun Fact #2: After independence from Britain following WWII, Singapore briefly merged with its big brother to the north, Malaysia. But thanks to racial strife between the Malays and predominantly Chinese Singaporeans, the island was kicked out in 1965. Singapore has gone on to become an economic powerhouse and first world nation while Malaysia currently ranks 79th in GDP. Whoops!
After eating my way around downtown, having coffee with some very pampered cats and strolling around the stunning Gardens by the Bay and exceptionally impressive Art-Science museum it was time to do some actual work. I spent the first two clinical days at Singapore General Hospital, in the emergency department with Dr. Marcus Ong and his staff. Here’s an excerpt from my Facebook travel diary with my first impressions:
“Spent my first day at SGH today. It’s a remarkably similar place, facing many of the same issues we do in the US. Grumpy consultants, slow throughput, ED boarding, and misuse of emergency services. That said, they see almost zero violent trauma, drug seeking is nonexistent, and psychiatric care is managed outside of the ED. Overall, the care is excellent and very up to date, with all the latest technology readily available but used in a more cost effective way.”
Efficiency is key. Patients are brought to private areas long enough to be evaluated and have any procedures done but are then moved to a holding area to maintain throughput. There is an observation unit for those needing a little more TLC.To combat the ever-present risk of communicable disease the city’s ERs have separate treatment areas for febrile patients. They learned this lesson from outbreaks of SARS, MERS and, most recently, Zika.
I was impressed with the care but noticed it to be somewhat less aggressive than what we do in the US, with invasive procedures done emergently if necessary, but more often left to be sorted out upstairs. While they see very little violent trauma, I was fortunate to see how they managed a motorcycle accident victim – a wealthy British businessman with broken ribs and a collapsed lung. At VCU he would have had a team of 12 providers standing-by on arrival, been stripped of every stitch of clothing and irradiated from head to toe by our CT scanner. At SGH he cracked jokes for an hour while a nervous intern tried his best to place a chest tube.
PSA in the subway station
Like everything else in the country, the healthcare system in Singapore is modern, effective and efficient (ranked most efficient in the world in 2014). Coverage is universal under the principle of no care being completely free which reduces wasteful over usage. Co-payments (typically 3-10% of the cost) and optional supplemental private insurance are paid from a compulsory personal savings account called MediSave. With the 3rd longest life expectancy worldwide Singaporeans spend just 1.6% of GDP on healthcare. For comparison, the US spends over 17% of its wealth on medical services yearly, and its citizens live just slightly shorter lives than the people of the Turks and Caicos islands at number 43 globally.
A cardiac arrest case, eventually with ROSC. Note the built in xray in the ceiling and LUCAS device in action. This is not a 3rd world nation.Waiting for admission in the ED
After my time in the hospital I spent a full day with the staff of the Unit for Prehospital Emergency Care (UPEC) which is led by Dr. Ong. Just a few years ago the government of Singapore sent experts around the world collecting best practices and poured tens of millions of dollars into the project, tasking UPEC with modernizing the EMS system. At the heart of that effort is the SCDF.
The Singapore Civil Defense Force is a quasi-military 4th branch of uniformed national service which includes both the fire department and ambulance service. Unlike the US, the two branches are almost entirely separate, with firefighters generally providing no medical care and responding only to fire incidents. One exception is the new “firebiker” program, with an EMT trained firefighter on a motorcycle able to respond quickly through traffic to cardiac arrest cases. The ambulance service, on the other hand, is well equipped and staffed by paramedics on every ambulance. A unique aspect of both branches is the inclusion of conscripts, young men completing their two years of national service. While most are drafted into the traditional military branches, others fill the ranks of the SCDF.
Morning inspection and roll-call at SCDF station Paya LebarDART – Singapore’s elite technical rescue/USAR team maintains 24/7 readiness for deployment anywhere in South East Asia.DART HRT – Heavy Rescue Tender, with a mission-adaptable, modular back half.
Fun Fact #3: There are two emergency numbers in Singapore. “9-9-5” is reserved for emergencies, with a government SCDF ambulance responding. “1-7-7-7” is available for non-emergencies, and staffed by unregulated private ambulance companies. Calling 9-9-5 for a non-emergency can result in a hefty fine.
I had a chance to spend time both aboard an SCDF ambulance and in their command center, where over 50 ambulances are dispatched to almost 1000 calls to 9-9-5 daily. Many unique challenges exist, ranging from the use of four primary national languages (English, Tamil, Malay, and Mandarin), to cultural and religious differences, not to mention a complex environment including dense urban centers and the surrounding swamps, jungle and sea. It was there I first heard the term “vertical response time,” the extra minutes which have to be factored in when lugging a stretcher and equipment to the 40th or 60th floor of an apartment or office building. To combat that particular challenge, the government has funded AEDs being placed in the lobby of every other housing complex as well as community hands-only CPR training, all organized by UPEC. The coordination of such an effort is a remarkable achievement.
Much of the same capability at a fraction of the costRed Rhino fire service QRV
UPEC/DARE – Community CPR course. The government aims to train 50,000 first responders in the next few years.
Fun Fact #4: The government LOVES fines. Jaywalking? $20. Smoking in an elevator? Better have $1000 to spare. Even drinking water on the subway or spitting out chewing gum on the street will set you back $500. But most Singaporeans will admit the loss of a few simple freedoms is worth it and has led to a safe and orderly society, with essentially no crime.
You don’t even want to know what they would do to you for eating a durian on the train.
As my time was coming to a close I had one last clinical opportunity, the one I was most looking forward to: race medical support for the Singapore Grand Prix. Now I’ve never followed Formula 1 racing, but if I learned one thing from the UCI Road World Championships in Richmond last year it’s that you don’t have to be a superfan to get excited when a big event comes to town. With an all-access pass, a chauffeured golf-cart, the scent of high octane gasoline and that distinct TIE-fighter whine of the engines I was soaking up an intoxicating atmosphere. The medical facilities were impressive, with the SCDF, dozens of volunteers from St. John’s Ambulance and the elite Disaster Assistance Rescue Team (DART) on standby. There were even fire-boats positioned to evacuate patients by sea if necessary, avoiding the inevitable gridlock of a city hosting a world-class event. Like everything else I came across during my time there, every detail was planned out and meticulously accounted for with robotic precision.
Ferrari 458s compete in the warm up to the Singapore Grand Prix
After the race, having completed my educational syllabus, I used my last day in the country to be a shameless tourist. The highlight was undoubtedly the stunning botanical gardens, a UNESCO World Heritage site. I spent most of the day strolling through various areas like the Evolution Garden, Healing Garden, Bonsai Garden and of course, the jaw-dropping National Orchid Garden. Next time you find yourself in the area, do yourself a favor and pay it a visit. You won’t be sorry.
The National Orchid GardenThe Bonsai GardenThe cable car to Sentosa island – in the distance, the whole world’s commerce passing through the Strait of Singapore
Although it may seem I was in a veritable utopia, by the end of my time there I was ready to come home. Not only was I missing my wife, but in a weird way the predictability of the orderliness, combined with the brutal heat became somehow… monotonous. Full of new knowledge and tremendous respect for the work being done to develop Emergency Medicine in Singapore, I caught the last seat on a full flight home after saying goodbye to my new friends at UPEC, SGH and the SCDF. Did I mention Singaporeans love abbreviations?
Dr. Ong and I
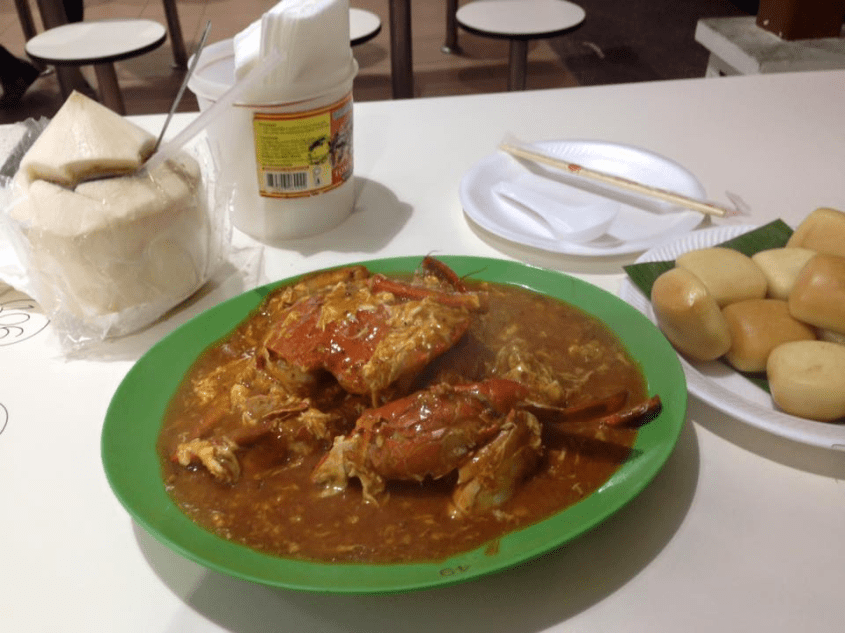
But what about the food?! Up to this point I’ve purposely avoided mentioning it to prevent an irreversible segway into what I can only describe as the best, cheapest, most diverse cuisine I’ve ever come across. It was simply too good for words, with each meal better than the last. Singapore more than lived up to its reputation as an international foodie destination, so I can think of no better way to conclude than with a stream of epic food porn. Enjoy!
~Amir
“Hawker centers” are Singapore’s answer to street food – delicious, clean and cheap. What more could you ask for?Bak Kut Teh – roughly “meat bone tea” – The most savory, flavorful broth with tender pork ribs. Sides include fried bread for soaking up the broth, various greens, a soy-sauce egg and braised pig intestine.Singapore Chili Crab – one of Lonely Planet’s “7 Iconic Dishes” worldwideBeef and Kailan greens with fresh sugar cane juiceBelieve it or not, this is a Michelin starred meal. Chicken Rice is just that – but better. On the left, roast pork two ways. Price? $5Fancy restaurant? Nope. This roasted Peking Duck is standard hospital food!The local coffee – “Kopi” – is thick and flavorful, sweetened with a dollop of condensed milk.Laksa – a rich Malay coconut noodle soup with various proteinsCurry three ways: Rice with chicken curry, fish curry, and tandori chicken. Roti bread to soak it all up.Grilled garlic king prawns with fried rice, greens and fresh mango juice.




")