

January 26, 2018
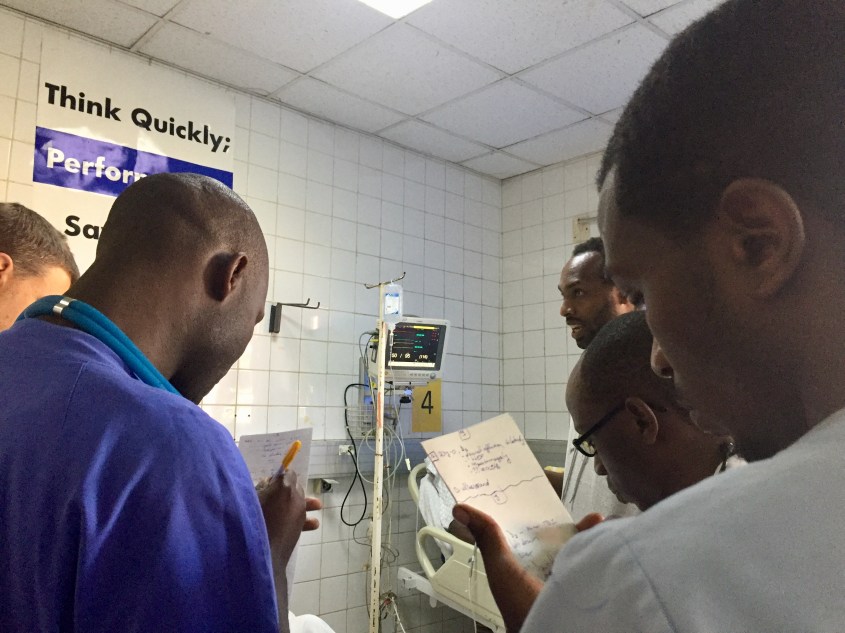
This morning Jane and I returned to Central University Hospital of Kigali (CHUK) to attend Rounds once again. Like Monday, we began in the RED Resuscitation room to see the most critical patients who arrived overnight.
In Bed 1 lay a man who initially went to a district hospital and had been transferred to CHUK just a few hours earlier. Previously healthy, about 3 weeks ago he began having fevers and then his whole body started to swell, which was followed shortly by trouble breathing. As soon as he arrived, the Emergency Medicine Resident performed a lung and heart ultrasound, and discovered fluid on both his lungs as well as a weak heart that didn’t squeeze as a heart of a man in his mid 30s should. I looked at the ventilator, and his oxygen reached only 85% at best. He’s likely suffering from a myocarditis. At home, this man would most likely be on ECMO, an advanced heart-lung bypass machine. Of course that’s not an option here, as ECMO isn’t even accessible in many places in the United States. His chances are slim if his oxygen levels do not improve.
Also in the RED room, we find a 10-week-old baby boy who suffered a severe TBI after a motorbike accident. Is it the same one my student was describing yesterday in class? The age is right, but this baby isn’t paralyzed. There must be two. Two 10-week-old babies with devastating neurological injuries after motorbike crashes. I can’t even imagine myself on one of these motorbikes nevertheless my infant daughter. I looked at the CT scan of the head and cringed – the skull was in 4 separate pieces, and somehow this baby was still alive.
Over in the YELLOW room, I discovered the same man I met Monday, with the fractured femur, but with no money to pay for the operation to fix it. His doctors have been struggling all week to find him help, as they don’t want to send him home with a fracture that, without repair, will likely affect his ability to walk. I inquired about the cost of the surgery, remembering the suggestion of Dr. Noah that we all chip in to help him. Dr. Joe, today’s EM Attending, explained that bills for services are usually rolled up into a single line item, making understanding and predicting the cost of specific medications or procedures extremely difficult. Sounds just like the US. “If I had to guess, around $100,000 USD,” he says. There goes the dream of us funding his operation.

We shuffle as a group to the next bed, when overhead we hear, “CODE BLUE, Room 9 – CODE Blue Room 9.” We walk with purpose back towards the resuscitation room to discover a man with metastatic liver cancer who is unconscious and not breathing. The residents jump into action, bagging the man while they prepare for intubation and the potential for CPR. The man’s family is close by, and the Senior Resident takes a moment to discuss with them goals of care, as CPR and ventilator support will likely not help this man with terminal cancer. He uses words and phrases provided by Dr. Noah in his End of Life lecture from Monday. The man stabilizes with the respiratory support provided by the Resident, and we return to rounds, goals of care still unknown.

After Rounds, Jane and I walked back to our hotel, stopping to photograph some sights and for “African Tea” at the Camellia Tea House . It’s a mix of ginger tea and warm milk, sipped slowly and served with a butter cookie. Yum.
Jane has been on the hunt for some traditional Rwandan music to take back with her. We can’t seem to find CDs anywhere. I’m unsure if that’s because like back home, CDs are a dying format, or if we just haven’t stumbled upon the correct store.

After shopping, we settled in for some lunch at our hotel. The food is good, but its appeal is more so the tropical balcony overlooking a busy intersection that lends itself to some excellent people watching. I’m cringing less each time as the motorbikes fly by, except when I see a baby on a mother’s back or a small child sandwiched between two adults on the same bike. There’s a stoplight at the intersection, but today it’s not in use. The convergence of cars, buses, motorbikes, pedestrians, cripples and cyclists is frenetic. I’m amazed there are no collisions. Back home in Richmond, our house too sits on the corner of an intersection, which despite much less traffic, has logged many more accidents and countless near misses.
Dr. Sudha arranged a lovely dinner at a restaurant with live music and traditional Rwandan dance to celebrate the conclusion of the courses for the week. Representatives from the Ministry of Health and Rotary joined us, as well as a few SAMU staff. Jane and I both wore African print dresses, because “When in Rome…,” right?
Tomorrow morning we are taking a safari tour to the Akagera National Park, just to the East, near the border with Tanzania. There’s potential to see leopards, lions, hippos, giraffes, zebras and more. We’re leaving at 6:00am to get there early before all the animals hide for the day.
~Steph
Explore more days in Rwanda:
Rwanda Day 1 | Rwanda Day 2 | Rwanda Day 3 | Rwanda Day 4 | Rwanda Day 5 | Rwanda Day 7 | Rwanda Day 8 | Rwanda Day 9 | Rwanda Day 10/11


9 thoughts on “Rwanda Day 6: More Motortaxi Morbidity”