These days, many people enter medicine as a second career. I am no different. I was an undergraduate business major and worked in the corporate world of internet marketing for 6 years prior to medical school. Perhaps a science major would have been more practical when I was spending 7 hours struggling to understand some fundamentals of molecular biology; however, my business background did occasionally give me a leg up. Going back to school at 30-something, surrounded by recent college grads, I realized a few lessons I picked up along the way weren’t necessarily obvious to others.
1. Everyone has a job, and they all matter
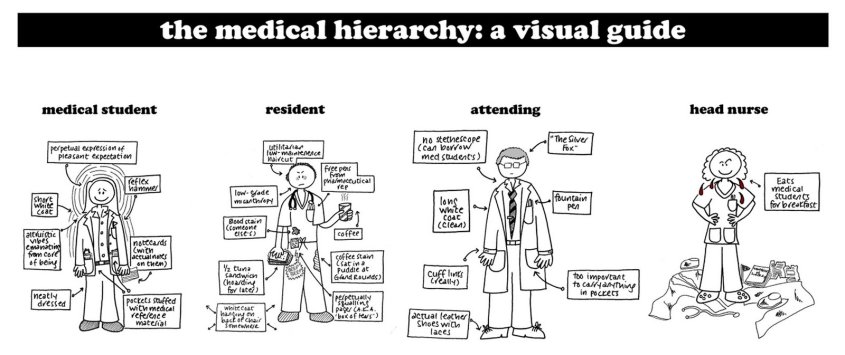
Despite modern movements away from it, medicine is an extremely hierarchical world. Medical students pine for that long white coat. Doctors bark orders at nurses without introducing themselves or asking nicely. Phlebotomists, lab techs, housekeepers and others largely go unnoticed.
One beautiful reality of capitalism is that jobs don’t exist unless they are vital… IMPORTANT. In medicine, we need janitors, doctors, accountants, secretaries. Everyone with a title has responsibilities and is therefore necessary for the organization to function. Companies with excess overhead from superfluous staff don’t stay in business very long (VA Hospitals aside). So when the surgical consultant steals a computer terminal from the ED Tech so she can finish her note, this disrupts work flow, and sends a message that somehow the doctor’s work is more important than the ED Tech’s. It’s just not true. Be mindful that everyone on the team has a job to do and people will want to be on your team.
2. “For-profit = evil” is not always the case
Yes, pharmaceutical companies are responsible for their reputations as greedy, evil, for-profit companies. Just ask Martin Shkreli. And while it would be great to provide free medications to any and all who truly have need, research and development (R&D) of new medications is risky and costs money. A lot of money.
On average, a new drug takes anywhere from 11-14 years to make it to market, and that’s IF the drug makes it that far. Of any new drug developed in a lab, there is an 8% chance that drug will actually make it to market, meaning it’s prescribed by doctors for actual patients.§ The money spent on R&D for 92% of unsuccessful drugs is a true cost, and those bills still need to be paid. Smart R&D focuses on modular development, so that one lesson learned developing a drug that failed can be applied to new research that will hopefully help a different drug get to market.
Yes there is excess and greed. Yes Big Pharma develops drugs based on profitability, not strictly based on need. People with “orphaned diseases” have to create non-profits and raise funds for R&D since the pharmaceutical companies won’t do it. It’s not ideal. Attracting the brightest minds to develop major pharmaceutical innovation requires paying people well, and I’ve yet to hear anyone tout how well-paid they are at their non-profit organization. In the end, it’s not as simple as saying “just lower the prices or make it free.”
3. Product perception is reality
Marketing is everything. You can have the best product in the world, but if no one knows it exists, or if consumers don’t understand what it can do for them, they won’t buy it. Similarly, you can get all the science right in medicine, but if results, diagnoses and plans aren’t communicated, getting it right doesn’t matter.
If anything this is even more applicable in medicine than business. While people have some innate understanding of what makes a good vacuum cleaner, they probably need more help understanding their liver failure and what treatment they need. I never assume patients understand their disease. Taking 5 minutes to explain the relation between the liver and ascites goes a long, long way.
4. Dress & Look the Part
Being a medical professional requires knowledge, honesty and altruism. Most people get that part right. But professionalism in medicine also means being on time, dressing professionally, and remembering that people are always watching. So for the EMT: put down the cigarette, tuck in your shirt and wear your gloves when needed. For the medical student: be the first one arriving to rounds, wash your white coat (not just once a semester either), lose the stubble and open toed shoes and ditch the piercings for the day. Doctors: wash your hands, put down your iPhone and give patients your undivided attention. All the knowledge in the world can be quickly overshadowed by a distracting or detracting exterior.
“The Doctor” by Luke Fildes
5. Listen to Customer Feedback
This is not “The customer is always right.” Medicine is different. Just because a patient thinks he needs antibiotics for his cold doesn’t mean he should get them. But your customers do know their bodies best and how they are feeling at the time. If you are handing a patient discharge paperwork and they “still don’t feel right,” stop and listen. In this case, the customer feedback is critical, and the price to pay may be high – both for the patient and for your wallet. Any seasoned Paramedic will tell you, “When the patient says they are going to die, I believe them.” We’ve all been there. And if you haven’t yet, it’s just a matter of time.
So that’s it, 5 small things. What lessons have you borrowed from an earlier career and applied to medicine?
In just two short months, thousands of newly minted young physicians will be walking into new hospitals, new jobs, and new responsibility. They’ll notice something unfamiliar tickling their calves on that first day – a long white coat having replaced the short one, which in our case went up in flames just days earlier. They’ll be excited and terrified, nervous and naïve.
A doctor’s “intern year” has become something of a legend in pop-culture, portrayed as twelve months of rude awakenings, sleep deprivation and verbal abuse, +/- a love triangle or two. Having been there, done that and proudly owning the t-shirt, I can say the reality couldn’t be further from the truth – at least it doesn’t have to be.*
To all the newbies out there – yes, there will be long hours and sleepless nights. You’ll occasionally go a full week without seeing your loved ones and eat whatever/whenever you can. Med school will seem a lifetime ago when you’re being asked at 3am what to do for a dying person, and you’ll wonder why they never taught you all the things that matter. But Steph and I have stumbled across the solution to all of that.
Champagne celebration for med school graduation | Photo credit: Amy McClure
We celebrate the small stuff.
Sure we popped champagne like we’d just won a Grand Prix on graduation day, but we’ve also raised a glass to finishing tough rotations, making a clutch diagnosis and running our first double cardiac arrest. We’ve made a ritual of rare Sunday mornings off together with a supply of cinnamon buns always available, just in case. Sometimes we just celebrate because it’s Tuesday and we can. By making a big deal of small victories, the roadblocks become surmountable.
Don’t get me wrong – residency is tough. In the past month, three of my patients have died, and I’ve told four others they have cancer. But for every bad day I have had there have been a dozen that left me thinking, “I have the best job in the world.”
I encourage all the newbies out there to approach this next chapter the same way. And remember: when the champagne runs out, there’s always more coffee.
I’ve had a few people ask me to write about this, so here goes. First off, my story is just that – mine and potentially not entirely applicable to others looking to change careers, but nonetheless I’m going to attempt to pull out the pearls and advice that I can. Here’s the step by step process I took to a total career and life change, from President of a boutique Interactive Advertising Agency, to Emergency Medicine Physician, in the span of 7.5 years.
STEP 1: Recognize you need a change
Sometimes the need for change is obvious – if you find yourself counting down the clock to the end of your workday, then something is likely wrong. What’s harder is recognizing the need for a career change when it’s less obvious – when you like the job you have, but you have more passion for something else. That was the case with me. I’d been fortunate enough to have great success in my last career. I was well-paid for doing interesting work with cool people. But, I had been volunteering with the rescue squad for 3 years and had gone back to school to get my Advanced Life Support (ALS) certification. I felt alive and intellectually stimulated in the course. I was finally getting to learn the deeper pathophysiology behind what I’d been seeing in my patients for the last 3 years. And, instead of volunteering the required 48 hours per month with my rescue squad, I was logging somewhere just over 100 hours per month. I was about to cross a threshold where I was spending just as much time pursuing my passion for Emergency Medicine as I was in my professional field of Interactive Marketing. That’s when I first had the idea of a career switch. That was October 2007.
STEP 2: Mull it over
A career change isn’t the kind of thing you should decide on a whim. So, do yourself and those around you a favor and take some time to digest the idea. One of the smartest things I did was asked my friends what they thought, “Could you see me as a doctor?” “Do you think I’d miss marketing & technology?” “When do I seem most happy?” If you have great friends & family like I do, they’ll have noticed this and be willing to share. For the record, my parents did ask me the night of my EMT-B graduation (December 2004), “Are you sure you don’t want to go to medical school?”
That said, be prepared that this is the stage where the naysayers also come out. I can’t tell you how many people said to me something along the lines of, “So I guess you don’t want marriage and kids then, huh?” To which I wanted to reply, “No, I’m pretty sure I didn’t say that.” The implication is reasonable though, and certainly something I took into consideration. At the time I was 27 and single with no kids. If I was accepted to medical school, would I ever have time to date? Even if I met the right person, would I be able to balance marriage, babies and a life as a Med Student/Resident?
But at the same time, was I going to put my dreams and my life on hold waiting for a theoretical knight on a white horse that might never arrive? I saw myself 10 years later without my knight or my dream career in medicine. I most certainly didn’t want to come up empty handed on both counts.
What about the financial implications? Here’s where it helped that I was single with no kids. Supporting just myself, I’d been able to save a decent lump of money while working. I was in a position to quit working and go back to school full-time (more on that in a bit). And if it meant going back to eating Ramen Noodles, it was just me who would have to suffer.
STEP 3: Gather Information
Having not been a pre-med major, I had no idea what the rules were for medical school. For example, would they even accept someone over the age of 30? What prerequisite courses are required? Does it matter that I majored in Computer Science, Marketing & Spanish and not Chemistry or Biology? What’s on this MCAT thing? Every career field will have some of these rules, written and unwritten. You need to know what you’re up against.
Do yourself a favor and do what I did. Make some appointments to meet with the people that matter. I had two major challenges: 1) identify and take all of the prerequisite courses and 2) understand admission requirements for medical school and assess my competitiveness. So, I knew I needed to talk to someone at an undergraduate university and at a medical school. Because I wanted to stay local, I set up appointments with the Dean of Sciences at Old Dominion University (ODU) and the Dean of Admissions at Eastern Virginia Medical School (EVMS). Getting the appointments was much easier than I had anticipated. I simply filled out contact forms on the websites for each school; they emailed me back within 48 hours. That was November 2007.
Also, this is a great time to network. On a side note, coming out of undergrad I was very hesitant to play the Networking game. I naively wanted to feel like I achieved everything I had on my own, without “cheating.” After working for a few years, I learned that success is actually a combination of three things: hard work, luck and help from those around you. Your neighbor may have gone to college with the Hiring Manager for the job you have your eyes on. Ask your Facebook friends if they know the people in charge at the place you want to go. Did you know you can search Facebook for people who work at specific companies? Simply type in “Friends who work at ________” and you might be surprised to find that someone you know works at the company or school where you need an “in.” Here’s an example from my page of “Friends who work at Google.”
The last thing I did as a part of my information gathering was organize what I had learned about the situation. A pro and con list if you will. It looked something like this:
STEP 4: Pull the trigger
This was actually the easiest step for me. By the time I reached the end of my Information Gathering stage, my decision was essentially made for me. So many people have barriers to making a big career change – no money for classes, family commitments, you name it – I had none of those things. I knew and still know so many people that would kill to be able to pursue a new life dream but can’t. Most of my CONS were just related to money. I couldn’t NOT do it.
STEP 5: Enjoy the ride
While med school was downright miserable at sometimes, ok many times, one thing I can say about this whole journey is that it’s been an amazing experience to help me grow as a person. I’ve learned a ton about myself, what motivates me, what I can survive. And, I feel true to my soul having pursued what at many points felt like an impossible dream. Oh, and the icing on the cake, I met and married my best friend.
Everyone warns you that Intern year is hard. It’s a year of little sleep; a rollercoaster of emotions both good and bad. Frustration and guilt in wanting to know everything NOW, because everything you don’t know might be what matters for this patient, this time. And trememndous successes. Some of the things I did this year, I really can’t believe I was able to do. And survive. Mostly, I’ve learned a lot about myself, and have been reminded yet again, that I work with an amazing group of people.
UP – Running a trauma when I thought I could never do it
I have a distinct memory of standing in the Trauma Bay at Norfolk General Hospital, watching the Trauma Team work its perfectly organized chaotic magic. I paid particular attention to the young female physician leading the whole thing – inserting an airway, calling out physical exam findings, doing an eFAST ultrasound to look for bleeding. I remember hoping, wishing I could ever have her confidence and calm demeanor. That thought was followed quickly by being thankful I wasn’t yet in that spotlight myself. I could never do that, right? In September I ran my first Delta Trauma at a Level I Trauma Center, and I survived to do it again.
VCU Medical Center Resuscitation Bay, Richmond, VA
DOWN – Those 2-week stretches not seeing my husband
I had no idea how much I need my husband to help me feel like a normal, healthy, centered human being. Amir and I had about four 2-week stretches this year where he was on nights and I was on days, or vice versa. One day we were so desperate for a date we coordinated a 20 minute coffee meet-up at the au bon pain in the hospital. Let’s not talk about what the house or laundry pile looked like during those stretches. This is the video we play each other if we ever need a pick-me-up:
UP – Procedures, procedures, procedures
Open Thoracotomy
Paracentesis
Lumbar Puncture
intubations, central lines, suturing, joint reductions, even a c-section… you get the idea. I get to work with my hands a lot.
DOWN – Crying in the ICU
So I’m a crier. Always have been. I have distinct memories of my dad trying to help me with math homework as a kid, me getting frustrated and crying (my stress response), and my dad getting frustrated because I was crying. “What’s crying going to solve?” he used to ask me, which of course, made me cry more.
To be honest, I was expecting to cry multiple times the first few months of residency. I actually made it to late February before it happened. Combine working 12-14 hours a day, 11 days in a row, with little sleep, food, potty break or non-medical human interaction (one of those 2-week stretches) – and now add to that a dozen of the sickest patients in the hospital. I broke down – red face, tears, snot, the whole nine yards. The nice thing about Intern year though is that everyone around you has been there, so I had about 4 senior residents plus 3 PAs sharing their crying stories right along with me to help pick me up. And that’s what you learn to do – pick yourself up, learn and keep going.
UP – Finally learning my way around the hospital (which is actually 4 hospitals)
Anyone who works in an old hospital knows how the building just gets added onto over the years, creating a behemoth maze of windowless hallways and floors that don’t match up. “Take the elevator to the 5th floor of North Hospital, turn left and you’ll be on the 1st floor of Main Hospital.” As if there weren’t enough to learn as an Intern.
DOWN – Cancer. I diagnose a lot of cancer.
I didn’t go into Oncology for a reason. It takes the smartest, strongest, most energized people to be cancer doctors. As an Emergency Physician, I expected to treat people with cancer, but I hadn’t thought of cancer as something I would diagnose. I guess I assumed that people would present to their PCP with concerning symptoms, get an outpatient workup and diagnosis by a specialist. But people do come to the ED for hematuria (blood in the urine), anorexia (lack of appetitie), back pain and weakness. And sometimes at the end of the workup, it’s cancer.
UP – Baby Mint Mochachino for a dying patient
Baby Mint Mochachino made with honor
I’ve seen a lot of amazing, caring people do a lot of touching things in the medical setting, but one moment stands out from this year. I had a patient who had chosen to pursue hospice care. He couldn’t stop telling me how beautiful his wife was and how he looked forward to seeing her soon. He had stopped eating and drinking days ago, so when he asked me for a “real coffee,” I was intrigued. He’d requested a cup of coffee from the medical student who poured him a cup of the hospital grade mud available to all employees. His dying wish was to have a real cup of coffee. How reasonable. I went to the ABP counter, told the story to the barista, and she whipped up the only coffee worthy of such a role – a baby mint mochachino, which she made with honor and pride in her work, even adjusting the temperature down to avoid any burned tongues.
So that’s it – Intern year is coming to a close, and July 1 I’ll be a “Senior Resident,” fraught with its own challenges and lessons to be learned.
Time is an interesting thing. Sometimes it feels as if it’s flown by, other times the same memory can seem quite distant – or both. For me, I can’t not write about an experience 10 years ago that’s left a forever imprint on me. And for the record, this was an experience that occurred outside of my EMS or medical duties, when I was spending time with friends in my own home (so it’s not a HIPAA violation). I’m writing about it because I need to, and because I want other people to know that critical incident stress affects everyone.
I had been in EMS right about the worst length of time. Not long enough to have any experience with a gunshot wound, but long enough to know how bad – how ridiculous, how severe and rare this all was. When he told me “5 people were shot point blank in the head. I’m pretty sure they are all dead,” I knew. I had been in EMS long enough to know those people were dead. To know that what was going on in my home was larger than anything Virginia Beach had seen in a long time. There would be tons of cops and SWAT teams and helicopters. I knew the enormity of what was amassing around me. I wanted nothing more than to see a familiar face with more medical experience than me.
A list of the charges against Marcus Valentino Garrett as a result of his actions May 28, 2005First off, let me say that I think about the people hurt and killed in this incident, while no longer daily, I’d still say monthly. Three young individuals at the prime of the lives were killed senselessly. No matter how much time I spend attempting to process this, that fact still perplexes and bewilders me.
I’m deliberately posting the unedited documents I have from the event (my written account of events, transcript of my call to 911) so you can appreciate exactly where my mind was at the time things were going on. I had been an EMT only 5 months, and this was the first gunshot wound I had ever seen.
Account of the Events of the Morning of May 28, 2005
1:00 am – I get home from airport and meet friends out at Luna Sea on 22nd Street
2:00 am – We leave Baja Cantina when it closes
2:10 am – We reach my condo at 315 24th Street. There were four of us present, myself, Jackie Johnson, Kristin Horgardt (male, unsure of spelling) and a friend of a friend, Shane. I got out my keys to open the door for all of us. We were coming in the 24th Street (side with our parking lot) entrance. We noticed that the residents of 110 were awake and partying. It’s normal for them to have their windows and drapes open with only the screen. Their cat usually sits there. Like us, they seemed to have been out at bars and were having a few drinks at their place after everything closed. The music was not tremendously loud. I only noticed male voices. No one was arguing; all seemed to be normal.
2:15 am – Melissa Ozmar, a girlfriend of mine, showed up downstairs for me to buzz her in. She had been out with us earlier, but drove a friend home and then came back. We buzzed her in without issue.
2:25-2:40 am – Melissa and I were out on my balcony that overlooks 24th ½ Street and the 25th Street parking lot watching people get their cars towed. Kris and Shane were in the living room watching a movie on DVD. Melissa and I spoke to a few people from the balcony. The only suspicious people we encountered were two guys that were a part of a group of 8-10 black guys. One of the two men asked us if he could come up and charge his cell phone. We found that odd and dangerous and said no. The other guy broke away from the group (that has been walking west on 24 ½ Street) and headed east back towards us. At the point Shane had come on the balcony, and the guy asked Shane if he knew where he “could get laid.” I jokingly said 17th Street, and the guy continued in that direction, away from his group of friends.
Kris and Shane decide that they are going to walk to the 7-11 on 24th and Pacific to buy cigarettes for Kris and candy for Shane. I asked Shane to pick me up a Payday. I told them to hit the buzzer when they got back and I would let them in.
2:45-2:50 am – After a quick 5-10 min max trip to 7-11, Kris and Shane hit the buzzer on the 24th Street entrance and I let them in. They walked right past Apt. 110 and did not notice anything odd. They sat back down on the couch to finish watching their movie. Melissa and I never saw anyone enter or leave the building through the 24 ½ street entrance. At least one of us was on the porch the entire time. No more than 2-5 minutes later, Kris called to me to tell me someone was knocking on my door. I went to the door and asked who it was. A guy told me he was hurt and needed to call 911. I opened the door and saw a young white male (John from CA) with blood on his hands and face. I told him to come in and sit down, that I was an EMT, and asked Melissa to dial 911 (2:55 am). I grabbed some spare gloves that I had and some clean washcloths. Patient stated that he had been shot. I initially could not find the entry and exit wounds. Melissa was a bit nervous and was not answering the call-takers questions well, so I grabbed the phone and relayed information to 911. I noticed a large amount of blood on the back of the patient’s shirt, so we removed the shirt. I was then able to see an entry would located behind the left ear, closer to the lymph node. I then located an exit would in the hair line, just left of the patients spine. I applied direct pressure while trying to minimize any spinal movement. The angle of the bullet was such that the wound appeared to affect only muscle tissue and not the vertebrae or skull. Patient’s ear was also bleeding. After examination, the bullet had grazed his ear before entering the neck. I then applied a second wash cloth to apply direct pressure to the ear. Patient complained of inability to hear out of left ear. Patient denied ever losing consciousness, denied back pain, shortness of breath or any other injuries.
During the course of treating the patient, he told me a lot of information about the events of the evening and what he saw. He told me he had been in the bathroom and his friends were in the apartment. He said the shooter shot him in the head and ran out of the bathroom. He did not see which way the shooter ran beyond that. He gave a vague description which I relayed to the call-taker: black male, mid twenties, dreadlocks to just above the shoulders. He said he recognized him from earlier in the evening when they were all out. The shooter knew Rachel, brown hair, a girl in their party (one of the people shot in 110). He did not know if tonight was the first time Rachel and the shooter had met or not. There was no argument between them early in the night that he saw. He did say that the shooter seemed attracted/interested in her.
He said that when he came out of the bathroom, he saw his four friends motionless on the ground, they had all been shot in the head. He was pretty sure they were all dead. He said he ran up to the 3rd floor to look for help because he thought it would be safer than going outside and was farthest away from Unit 110. He also remembered that the gun was “squared off” at the end.
3:00-3:05 am – Police arrive and bang on my door. We open it, and they search my apartment for the shooter. A lead officer asked me if I had any medical training, and I let him know I was an EMT with Station 14. I gave him a status update on the patient’s condition, and the SWAT Medic arrived very soon after. The medic quickly assessed the patient and asked me to remove pressure so he could see the wounds. He then called for a c-collar from 1421 to be brought up to us. We applied gauze to the wounds and secured the patient’s neck with the collar. Scene was not safe, so backboarding was not an option. SWAT Medic walked the patient down the stairs and out to the ambulance.
3:10-3:15 am – Medic knocks on door again to verify that patient never lost consciousness. Medic stated that he was now having CNS issues. Medic also asked me not to dispose of any of the towels or gloves used to treat the patient.
I gave a verbal account to two detectives around 7 am and 12 am respectively. The second detective collected the patient’s blood-stained shirt, which had been lying on my kitchen counter. She interviewed Kris and me, and asked that I write an extremely detailed account of the events.
911 Transcript
The following is a taped 911 call between Virginia Beach Communications Dispatcher Charles M. Simpson and caller Stephanie Krebs [Louka], which occurred 05/28/05, 02:56 hours reference DR# 2005-031807. Victim JKT can be heard in the background.
CS: Dispatcher Charles M. Simpson, SK: Stephanie Krebs, JK: JKT
CS: Virginia Beach 911, where’s the emergency?
SK: Hi, um, we are – Apparently there’s an individual that’s come upstairs –Hi, my name is Stephanie Krebs. I’m actually an EMT with Virginia Beach Volunteer Rescue Squad.
CS: Where are you at?
SK: Um, I’m at 315 24th Street
CS: And what is wrong there?
SK: Um, I live in apartment 320 on the 3rd floor. Can you get me a towel? Sorry, a guy just came in. He’s telling me that there were four people on the first floor. Um, the man that’s here that I’m treating right now – Now what happened to you? That man treating, that I’m treating right now is bleeding from the back of the neck. Do you know how – what the status of the people on the first floor is?
JT: (inaudible)
SK: He said that the people downstairs on the first floor were shot in the head.
CS: Do you know if anyone is alive or, what status is on anything?
SK: Um, did you, did you see the people downstairs? Was anyone alive or…
JT: (inaudible)
SK: People were shot in the head. They don’t seem to be moving. The guy up on the third floor here. He’s talking to me. He’s conscious, breathing, um, doesn’t seem to have neck or back pain. Um –
JT: (inaudible)
SK: He can’t hear out of his left ear.
JT: (inaudible)
SK: No, that’s okay. Did you know the people downstairs?
JT: Well, I just came in from California. They’re my friends from college.
CS: Do you, do you know anything about the status of them?
SK: Um, I, I don’t and obviously _________I’m not gonna go down there. Um, he said he thought they were all shot in the head, four individuals.
CS: Do you know anything about who did it?
SK: Do you know who did it at all?
JT: No.
SK: You just saw the people?
JT: One guy.
SK: It was one guy. Did you, did your friends know them or…
JT: No.
SK: No.
CS: Can you tell me what he looks like, where, where he went?
SK: He thinks it was someone they had met tonight. Was he black, white?
JT: Black.
SK: A black guy. Do you know how old?
JT: Maybe mid 20’s.
SK: Mid 20’s. Did he have any tattoos or piercings?
JT: Um, nothing ___________.
SK: Dreads or maybe dreadlocks to about shoulder length.
CS: Uh, ma’am, I can’t hear you.
SK: I’m sorry. Um, the shooter seems to have dreadlocks about shoulder length.
JT: (inaudible)
SK: Sure they’re coming right now.
JT: (inaudible)
CS: Okay. Anything else about his dress?
SK: What’s that – Do you know what he was wearing?
CS: He’s on the third floor with the caller I’m – Not the – I mean the victim. One of the victims is. The suspect I’m trying to get information on.
SK: Sure. Um, the one __
CS: Ma’am, where did the guy go? Can you tell me that, anything?
SK: Did he – Which direction did he run – Did he run out 24th ½?
JT: I don’t know. I was in the bathroom when ________________.
SK: ______________.
CS: So he don’t know where he went?
JT: __________shot me___________.
SK: Okay. Where did he shoot you? I think he grazed you. Hang on for a second. Melissa – Hey, buddy, I’m gonna have to cut your shirt off, all right.
CS: All right. Listen, the guy that’s with you, where is he hit at?
SK: Um, I’m – That’s – I’m gonna cut off his shirt right now ‘cause I think it’s – He’s not bleeding too severely. If you can take it off –
CS: Can you tell me from where?
SK: Yeah, I’m looking right now. It’s not visible. He says he got shot, but.
CS: In the torso area, head?
SK: No, no, no, no he has like a small ________ on his lower head.
CS: _____________.
SK: Actually, I see the entry wound, and he’s very lucky. He got grazed. He has an entry wound.
CS: Where?
SK: On his – It’s just below the patient’s left ear, and it’s probably entered and exited only through about one inch of skin.
CS: And you, and the guy has no idea where the guy did the shooting went?
SK: No, he – He was using the restroom.
CS: All right. Does he know why the guy did it?
SK: Where he did it?
CS: Why? Why did the guy shoot them?
SK: Um—Do you know—I know you said you thought you met them earlier in the evening.
JT: (inaudible)
SK: Uh huh.
JT: (inaudible)
SK: Do you know what it was about?
JT: No.
SK: Uh, apparently one of the women in the –
CS: I’m trying to get information.
SK: Okay. Apparently–________dispatcher—–
CS: Male subject shot just below the ear. He’s on the third floor.
SK: They’re coming in here.
CS: Let me know when police get there.
SK: Okay. Can someone go down to the, um – Well, actually never mind, don’t, don’t, don’t. Don’t go down.
JT: (inaudible)
SK: Okay. Can you – Is the door locked?
CS: _______________.
SK: You locked them, okay? Um, apparently, the, um –We’re not sure of the motive of the shooting, but the assailant was talking to a woman named Rachel earlier who is a brunette, long curly hair. Um, they had met earlier in the evening and didn’t know each other prior.
CS: And the shooting started, uh, while they were talking to her or do you know where Rachel is at?
SK: Uh, we think she might be one of the victims on the first floor. Are you sending, um, Station 14?
CS: Yes ma’am, we got. I don’t know what rescue unit. Just a moment, I’ll check.
SK: Okay. Sorry. I __________. I’m supposed to be on duty tonight. ________ my shift.
CS: Yeah, 14____ should be there.
SK: Okay.
CS: I imagine they’re all pretty much –
SK: They’re probably –
CS: –downstairs waiting for police to clear them.
SK: Sure. Sure. Um…Actually, there’s – Hey Melissa – Will you __________the cops out there. Yeah, let ‘em know it was 110.
CS: What is 110?
SK: 110 is the apartment number where we believe all the victims are.
CS: What about your apartment number?
SK: I’m in 320.
CS: On the third floor?
SK: Correct. And – Hey, Kris, can you make sure that deadbolt is locked on my front door. We got –Who is it? Lock the door. Okay.
CS: Now, I’m getting a little ____________.
SK: Who are you? 110.
CS: Who are you talking to?
SK: Police are here now.
CS: The officers are there.
SK: Okay, is it okay to hang up with you know?
CS: If you are with the officers, yeah.
SK: We are with officers.
CS: All right. Well, thank you for your help.
End of recording.
I’ve learned a lot from this experience, in no particular order of importance:
After the police leave a crime scene, you are on your own. What they never show you on TV is that after the crime tape is peeled away, the blood and biological hazards are left for the property owner to address. There are private cleaning companies that drop off fliers and business cards at murder scenes. Sort of like ambulance chasers, I suppose. The expense belongs to the property owner. Many insurance policies have exceptions for acts of violence, so owners have to pay out of pocket.
Police carry more than one type of gun. Anyone that knows me knows that I hate guns. I literally cried the first time I saw one at a neighbor’s house in 6th grade. I knew police carried handguns on their hip, but I had no idea they also carry machine gun like rifles. Big guns. Big guns in my house, opening closets, looking in my dryer for hidden threats.
Memory is fallible. As the case went to trial, I was called in by Harvey Bryant and Colin Stolle for witness prep. I would have bet you $10,000 that I had a full, vivid recollection of the events of that night. They felt so vivid in my mind I assumed they had not faded or twisted. To jog my memory, they played the audio of my call to 911 and showed me photos of JKT’s injuries. I was wrong on a few small things, and it will forever make me question witness testimony in court.
Trials and long and exhausting for all involved. Companies are required to allow employees to attend jury duty, but there’s no provision for people who are subpoenaed as a witness. Some companies cover witness testimony if it’s company related, but most do not. Good Samaritans who attempt to intervene can be rewarded with mandatory court appearance, without pay or protection of their jobs. Fortunately I was able to negotiate my contract with Launch Interactive to include paid leave for testimony in the trial. I imagine not everyone is so lucky.
I’m pretty good in an emergency. I know this sounds silly seeing as I’m now an Emergency Medicine Physician, but 10 years ago I was an inexperienced EMS provider that had never really been put to the test under stress. When I listened to the 911 call, I was surprised and a little proud of myself in how clear and calm I seemed. That’s certainly not the way I remember feeling.
Amber Alerts save lives beyond just the kidnapping victim. The way Marcus Garrett was ultimately apprehended was thanks to an Amber Alert. On his way to flee, Garrett scooped up his daughter, activating an Amber Alert across the state. A law enforcement officer, aware of the alert and on the lookout for Garrett’s car, ultimately apprehended him. Who knows how many lives that officer may have saved that day.
“Maximum Security Prison” is no cake walk. After his conviction, Garrett was sentenced to life in prison at Red Onion State Prison in the most western part of Virginia. For years I pictured in my head, Garrett shooting hoops on a basketball court, chatting with fellow inmates at a lunch table, meeting with visitors behind a clear plastic wall. Like on TV. VCU Medical Center, where I work, has a whole secure floor dedicated to inmates. One day I heard a guard mention he worked at Red Onion. Curious as to the actually quality of life there, I asked. Apparently they spend 22 of 24 hours in a day locked in solitary confinement with no windows, no activities, no interaction with others, but LOTS of time to think. Huh.
So how do I feel about everything now? It’s still hard to say. My thoughts are still all over the map.
I do know that I’m glad I opened the door that day. JKT ended up getting married and has since had children. That makes me smile. When I met with Bryant and Stolle, I learned just how close my friends and I came to being victims ourselves. That’s a thought I tuck way way back in my head and prefer to forget whenever possible. And most of all, I still want to know “Why?” Cliche I know, but I really am curious what motivates someone to do such a thing, or allows them to lose control and change the course of history for so many good families. I admit that on many occasions I’ve Googled Garrett, his prison, his status, his contact information. I worry about myself that I’d ever want to reach out to such a creature, even if to gain closure for myself. I’m not sure what I’m looking for, but I’m pretty sure I’ll never find it.
Lastly, I do want to thank John Carey and Norvel Allen for looking out for me after this happened. Since I wasn’t technically on duty for this event, I wasn’t included in the Critical Incident Stress Management debriefings that took place after the shooting. When I drive around Virginia Beach, I can point to a hotel where a woman overdosed on heroin at her best friend’s wedding; the roadway where 3 kids were driving too fast and paid the ultimate price. After 10 years in EMS, nearly every block has a story. I think everyone in public safety does that, 911 dispatchers included. But it’s different when it’s your home. You leave for work and still can’t help but look at the oddly cut out square of carpet that replaced the original bit that was soiled with an 18″ diameter and 2″ tall pool of clotted blood. You come home and retrace those same steps you took that night – passing by that window with celebratory voices, yet now so silent. You get an at least twice-a-day reminder of the horror and violence that entered your home that warm Friday night. It’s never normal, just slightly less obvious. On this 10 year anniversary I hope that the families of all involved find peace and warmth.













 I actually made it to late February before it happened. Combine working 12-14 hours a day, 11 days in a row, with little sleep, food, potty break or non-medical human interaction (one of those 2-week stretches) – and now add to that a dozen of the sickest patients in the hospital. I broke down – red face, tears, snot, the whole nine yards. The nice thing about Intern year though is that everyone around you has been there, so I had about 4 senior residents plus 3 PAs sharing their crying stories right along with me to help pick me up. And that’s what you learn to do – pick yourself up, learn and keep going.
I actually made it to late February before it happened. Combine working 12-14 hours a day, 11 days in a row, with little sleep, food, potty break or non-medical human interaction (one of those 2-week stretches) – and now add to that a dozen of the sickest patients in the hospital. I broke down – red face, tears, snot, the whole nine yards. The nice thing about Intern year though is that everyone around you has been there, so I had about 4 senior residents plus 3 PAs sharing their crying stories right along with me to help pick me up. And that’s what you learn to do – pick yourself up, learn and keep going.




