

Traction splints have been around since the late 1800s and were first employed during WWI. Given the lack of alternatives and atrocious environment, they were credited with massively lowering the mortality rate of soldiers suffering femur fractures on the battlefield. The idea was simple – take the long, sharp shards of broken bone, which exist within millimeters of the largest artery in the body, and stabilize them to ease pain and help control or prevent massive bleeding.
A century later, little has changed. There are a few basic flavors, but all have the essentially the same design of a long rod that runs against the affected leg and something which with to pull tension upon and secure the foot or ankle. Despite a lack of continued innovation and even less in the way of empiric research, an almost identical device to that which made its debut with the British Army in 1915 is required aboard every ground ambulance in the country. And almost every one of them resides in a cabinet or under a bench, forgotten and ignored until the biennial state inspection rolls around.

All EMTs are taught the procedure for applying a traction splint, but too often it is done in the classroom then never again. In my own experience of almost a decade of EMS, I have had the opportunity to apply one only once. As an ER physician for the last three years at the largest, busiest trauma center in Virginia, I have yet to have a patient arrive with one in place. My theory is that providers often do not consider it when appropriate, and even when they do their familiarity and comfort with the procedure is lacking, so it is skipped. In fact, one study found them to be applied in only 38% of appropriate cases and of those, 2/3 were placed incorrectly.
In other words, if you happen to break your leg, there is only about a 13% chance someone will correctly stabilize that razor sharp bone jostling against your femoral artery while you bump along to the hospital.
Since accurately practicing the procedure without crippling and otherwise healthy recruit is difficult, I looked up available traction splint training models. They cost around $1800, and are full of unnecessary bells and whistles, well beyond the means of many small EMS agencies. So I took matters into my own hands and created a rugged, reliable, anatomically and physiologically accurate model for less than $75. I’m offering it here, open sourced, to anyone who may want to replicate it for his or her training department.
You will need:
Tools:
- Standard drill
- Manual or electric saw
- Measuring tape
How to:
- Rubber exercise bands were stretched along the length of a two foot long section of 1 ½” PVC pipe, using duct tape to secure either end. The pipe was then cut diagonally in the middle, simulating a fractured bone.
- A six-inch section of the mannequin’s thigh was removed.
- Matching holes were drilled in the proximal and distal sections of the “broken femur” and the mannequin leg.
- The simulated bone was inserted and secured at both ends with long zip ties passed through the holes.
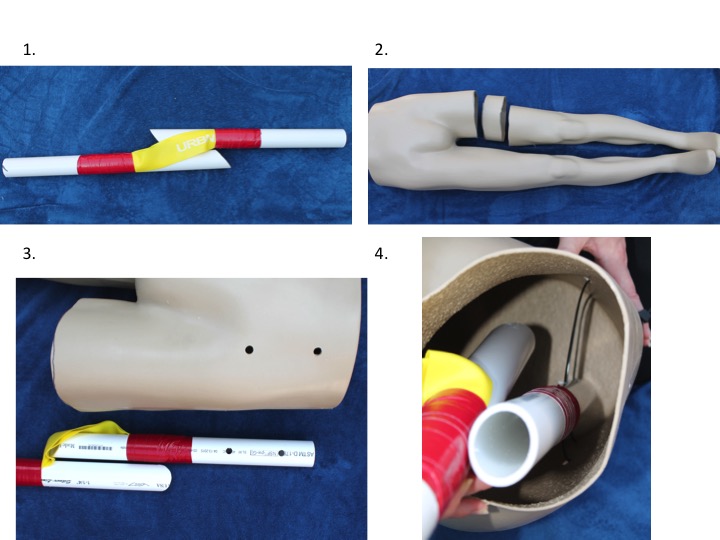
At rest, the proximal and distal segments of the mannequin leg fit together, accurately simulating the shortened extremity one would expect with such an injury. The exercise bands create a physiologic level of tension, and the leg can be pulled to length and stabilized using any commercially available traction splint. At length, the gap created allows the learner to visualize the physiology of the injury and intended function of the device.

If you do make one, please post a comment and let us know how it turned out!
~Amir

(The concept for this model was presented at the National Association of EMS Physicians annual conference in New Orleans, LA as an educational innovation on Jan. 24, 2017).
- American College of Surgeons (2009). Equipment for Ambulances. https://www.facs.org/~/media/files/qualityprograms/trauma/publications/ambulance.ashx
- American College of Surgeons (2012). Chapter 8 Musculoskeletal Trauma. Advanced Trauma Life Support Student Manual. 219-220
- Abarbanell, N. (2001) Prehospital Midthigh Trauma and Traction Splint Use: Recommendations for Treatment Protocols. American Journal of Emergency Medicine. 19 (2). 137-140.
- Skelton MB and NE McSwain (1997). A Study of Cognitive and Technical Skill Deterioration Among Trained Paramedics. Journal of the American College of Emergency Physicians. 6 (10). 436-438.
- Daughtery, M., Mehlman, C., Moody, S., LeMaster, T., & Falcone, R. (2013) Significant Rate of Misuse of the Hare Traction Splint for Children with Femoral Shaft Fractures. Journal of Emergency Nursing. 39. 97-103.


I presume all those battlefield femur fractures were from GSWs?
LikeLike
Definitely the majority. The machine guns were set up at about knee height, with troops walking into the hail of bullets. But also had artillery shells going off everywhere, so some blunt trauma and shrapnel too. Pretty hellacious.
LikeLike