Right now there’s a whole new crop of medical school students graduating in a month who will start their careers as doctors on July 1. There are two things every medical student looks forward to receiving as an Intern – a long white coat and a pager. But any Resident will tell you: after your first night on call, you want to throw that pager against the wall and then stomp it into little pieces.
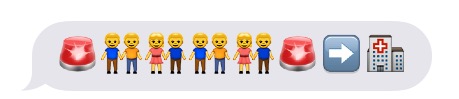
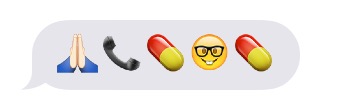
But what if pages, instead of boring B&W text, arrived as an emoji puzzle to decipher? That just might make getting 84 pages in a 12 hour Trauma shift slightly more tolerable. See if you can figure out these common pages.
The “Frequent Fliers” of Pages
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Answers to “Frequent Fliers” Pages
Mrs. Jones has a headache, please order tylenol
Mr. Smith has post-op pain, please increase his pain meds
Code Blue, Mr. Jones
Please renew Mr. Smith’s order for restraints
Mrs. Jones needs a diet order
Baby Davis is febrile and has no PRNs
Mr. White needs zofran for nausea
Another ED admit
The transfer from the OSH is on the floor
Please call Pharmacy, you messed up your order again
Who is going home today? -Bed Flow
Mr. Smith needs a laxative
Mr. Jones needs CIWA scoring
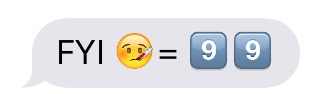
And, just for fun, some not some common but ridiculous (and true) pages:
FYI: 3AM page for a “fever” of 99.0F
Mr. X had a nightmare. He’s awake now.
Add your own favorite pager stories (and emoji puzzles) in the comments!
Yesterday I attended the 17th Annual Rao R. Ivatury Trauma Symposium hosted by VCU Health. I took away multiple “nuggets” to incorporate into both my prehospital and ED practice. The conference is geared towards anyone taking care of trauma patients – not just doctors but nurses, social workers, nutritionists, therapists and EMS providers, too. I highly recommend checking it out next year. Save the date: Wednesday, March 29, 2017.
Always a leader in EMS advancement, members of the Richmond Ambulance Authority (RAA) presented a poster on delivering “Good Medicine in Bad Places.” To the credit of RAA, they have developed a council with their partners in Police and Fire, to address regional response needs to unique and dangerous situations (i.e. active shooters, bombers, terrorist attacks). The data they presented is accurate – the number of incidents is rising, and the fatalities climbing.
Tactical Combat Casualty Care (TCCC) is specialized training that originated in the military. TCCC is currently being tested and studied in the civilian public safety setting. The TCCC conversation is an important one. Specialized training for these situations is an unfortunate necessity in the United States. A little background info on how these things are currently handled – most cities have specialized SWAT Medic teams comprised of talented, elite individuals adept at not only the delivery of prehospital medicine, but also in things like shooting, hand to hand combat and law enforcement. These providers are a special breed – in most cases considered the best of the best in their public safety organizations. I’ve been hearing the rumble and chatter over the last year, and it was again echoed by RAA yesterday. There is current shift in conversation towards training 100% of EMS providers to enter the warm and hot zones, to render care to patients while under fire.
It’s well known and proven that the current model of Fire/EMS waiting to enter scenes causes treatment delays that increase patient morbidity and mortality. In the December 2015 issue of the Journal of Emergency Medicine, Peter Pons of the Hartford Consensus commented that “fire/rescue and EMS personnel must work with law enforcement agencies to enter these scenes earlier than has been traditionally performed, intervene promptly to stop ongoing external hemorrhage, and incorporate basic concepts of tactical combat casualty care/tactical emergency casualty care into their education, training, and practice.” I don’t disagree with that, but I’m not sure it makes sense for us to immediately assume ALL Fire and EMS personnel should be entering scenes with active shooters – as if it’s simply one more bullet point we can just tack onto the job description.
If you think about our existing public safety system, some firefighters enjoy both patient care and fighting fire, while others if given the choice, would only ever fight fire. Similarly, some Fire and EMS providers might be part cop/soldier at heart – both capable and interested in taking on TCCC. I can assure you that not everyone on an ambulance has that police/soldier side that wants to run into an active shooter scene. Yes, EMS is a dangerous job; I’ve been punched and had a knife drawn on me in the back of the ambulance (no one tell my Mom please). Of course you can never predict what may happen and need to be ready for anything. That’s not what I am talking about in this instance. What I’m saying is that if a call goes out for an active shooter, it might not be wise to require 100% of the Fire and EMS personnel to be able to enter that active scene. Here are just a few reasons I think that could be a bad idea.
Figure 1: Crossover of skills/interests in various professional fields
Negative Effects on Recruitment
As I mentioned, not all EMS providers want to take on the police/military type role of being armed with a weapon, entering dangerous scenes and providing care under fire. I don’t know how big of a chunk of people that is, as it hasn’t been surveyed yet to my knowledge. I can say personally, having been in a building with an active shooter, I have zero interest in doing so again, even with the most state of the art training. How many of the 840,000 certified EMS in the US might we lose if that bullet point gets added to the job description? Additionally, 22% of those 840,000 certified EMS personnel are volunteers. Some volunteers might want to play a part in TCCC, but if you have a family and derive no paycheck or medical benefits from your volunteer EMS gig, can you really afford to enter that scene? And what will become of all the career providers who want to do patient care, but don’t want to risk their lives. Perhaps we will we see them shift into the hospital in ED Tech, CNA and RN roles.
Distraction Away from the Medicine
Even right now, EMS education has two large components: 1) the medicine, taking vital signs, deciding what drugs to give and when and 2) operational aspects, entering a scene safely, driving an emergency vehicle, operating a portable radio, etc. As an ED Physician, I admit my bias towards the importance of #1. We’ve all had the trainee who wants to drive lights and sirens before he’s mastered taking a blood pressure. With only ~160 hours of instruction in the current NREMT course, I worry that adding the required training for TCCC will shift focus away from the medicine and negatively impact patient care, potentially leading to more morbidity and mortality across all patients, improving outcomes for those victims requiring TCCC, but leading to a net decline in overall care. Perhaps the solution will be increasing the course length. I’m not saying it can’t be done; I just hope someone studies and considers that before implementing blanket curriculum changes.
Are EMS Providers Physically Fit Enough?
Sadly, three quarters of active emergency responders in the US are overweight or obese, and 75% have been diagnosed as hypertensive or prehypertensive. All in all, we are not a healthy bunch when compared to our counterparts in Police, Fire and the military. How many EMS providers will meet the physical demands required for TCCC? Even if people want to take part in TCCC, will they meet the physical requirements to do it safely, or perhaps be pushed out of a job they love, despite providing excellent medical care.
Would it actually improve care?
To justify the risk associated with TCCC, you must be able to prove that more lives would be saved than lost, and not just during active TCCC situations, but across prehospital care as a whole. It just hasn’t been studied yet. Perhaps once studied, it will prove to be net beneficial, but right now we just don’t know.
So those are my thoughts; I’m curious to hear yours.
The great thing about a British theme is you can apply it to most types of parties. Whether you are throwing a baby shower, birthday, bon voyage, or simple dinner party, the theme is flexible and can be expressed in a number of creative ways. My husband is 1/2 English, so we decided to throw a England/London/British themed Valentine’s Day party and called it “Love in London.”
Food
British food has a reputation for being a little dull and boring, but your spread doesn’t have to be. There are so many amazing recipes online, it can be hard to decide just what to make. We opted for sausage rolls, beef wellington (labor intensive & expensive, wouldn’t do it again), fish & chips (just buy ’em & fry ’em), cucumber & tomato salad, cucumber sandwiches and more. You can add some easy flare to your finger foods with these union jack toothpick flags.
Simple sausage rolls with union jack flagsMarinated cucumbers, onions & tomatoes add a flavorful vegetable dish
Last but not least, don’t forget proper condiments for your amazing food. Buy a bottle of malt vinegar for your fish & chips, and a bottle of HP sauce, and you’ve got your bases covered.
Don’t forget the condiments!
Drink
Ok, depending on your crowd, this might be the most important aspect of the party. There are lots of great drink options, but a British party wouldn’t be complete without Pims cup. There’s no exact recipe you have to stick to – I like taking whatever fruit looks fresh at the store and adding it to Sprite and/or ginger beer. For ease, you can also mix up a whole pitcher to have ready to go, similar to a sangria.
A spin on the traditional Pims cup
Fortunately we can thank England and Scotland for having a number of great beers. Head to your local beer/wine outlet and find the “England” section. We went to Total Wine. You only need a 6-pack or so of each if you are buying a big selection. Guests enjoy trying new beers as well as old favorites.
If you want to try something really special, and have some time to plan ahead, take a chance on a home brew and create your own. We made a delicious London Porter in just 4 weeks using this easy home brewing kit. We also customized the bottle to fit our theme using these handy waterproof labels for your home printer. We sealed the caps with union jack flag stickers for a finishing touch.
London Porter Home Brew
Dessert
There are many creative options for desserts to fit your theme. I’m not much for baking, so I cheated and outsourced a bit of this. The classic English dessert is a trifle, which is simply a layered dessert, typically with pudding, sponge cake and fresh fruit.
Strawberry trifle with fresh berries
The hallmark of English tea time, after the tea of course, is small cookies. Any small simple butter cookies will do. You can make these, but I opted to buy pre-made. For a mixed display, buy a box of chocolates to add to your 3-tier cake stand, and you’re ready for tea time.
Traditional 3-tier cake stands with tea time floral designsStore-bought coconut macaroons on the bottom tierAdd a frilly tablecloth to complete the authentic tea time look
For another dessert option (which is a great go-to for any party or theme), consider some custom decorated cookies. These sugar cookie masterpieces are from Cookies by Design in Virginia Beach. They are also a hit if you have little kids attending your party.
Hand-painted London themed cookies by Cookies by Design
Decorations
The easiest way to convey “British” visually is with the union jack flag. You don’t have to be an artist to create cool and creative decorations. Add a $5 union jack flag over a white tablecloth to create a bold canvas for your delicious food.
Another option that requires no artistry, is to apply this $4 union jack duct tape to simple objects. For this project, buy 3D cardboard letters to spell whatever you choose. Then wrap them in the duct tape and viola!
“LOVE” decoration made with 3D letters and duct tape for just $8
If you do consider yourself artistic or crafty, and don’t mind putting in some time cutting objects out, consider making your own garland. Find any image you like online, print it on photo paper, cut it out, hole punch it and string them together. Add a lace paper doily for an extra English touch.
“Love in London” hearts strung together with lace doilies and twineItty bitty hearts strung together with silver thread to make a precious garlandTemplate for tea time heart garlandSearch your house for any knick knacks that fit your theme and display them togetherColorful tissue poofs are cheap and high impact
Music
Pandora has an array of great themed channels. The best fit for an all-ages England themed party is British Invasion Radio.
Games & Fun
Party games and activities are tricky. Everyone’s been to a party where games feel forced and grueling, but you don’t want a party with everyone just standing around. Two simple activities I love are photobooths and trivia. They are great because guests can participate on their own time throughout the party, and they don’t take any bandwidth away from the host or hostess.
Photobooth
Grab some simple props (hats, glasses, boas) and if you want to go big, a life-size celebrity cut-out. Kate Middleton and Queenie were the life of the party.
If you entertain a lot, consider investing in the modern polaroid, the FujiFilm Instax mini camera. It instantly prints a polaroid-style photo that makes a great takeaway memory for your guests.
Trivia
Create a set of questions related to your theme and post them, along with pens and ballots, for guests to fill out. Winner gets a prize!
So that’s it, ideas for food, drinks, music, decorations and activities for your next London/British/English themed party. For additional ideas not mentioned here, check out the Love in London Pinterest board.
On July 4, 2013, Dr. Paul Aravich joined TeamLouka on the ambulance as an observer. He was asked to jot down a few thoughts on his experience. His essay is shared below.
~Steph
Reflections of a Virginia Beach Volunteer Rescue Squad Lay Observer, July 4, 2013.
Paul F. Aravich, PhD Stephanie Krebs and Amir Louka are two VBVRS volunteers and EVMS medical students who are “social change agents and leaders for the greater good of the community.” They invited me to run with them at Station 8 on Independence Day, 2013. I saw 2 other EVMS students that day who I also admire: an exceptional paramedic who is a new medical student, and a Navy veteran and physician assistant student who is as gentle as he is tall. I witnessed great respect between VBVRS, fire department and ED personnel in almost every instance. And I saw cutting-edge wireless technology and state-of-the-art equipment—although I am still not sure if it the ambulance is a box or a truck.
At the station I hung-out with a volunteer from York County who served at the World Trade Centers and Katrina, a new EVMS graduate student, a senior volunteer who is a builder of persons as well as of homes and barbecues, a critical care nurse from Chesapeake, and an accountant. We talked about abandoned older persons, defensive medicine, how to read an ECG, challenging behaviors, not getting T-boned at intersections, altruism, family, political turmoil in Egypt, and who catches a baseball better, the bulked-up waiter at IHOP or a nerd like me who, like Winnie the Pooh, is actually a “bear of little brain.” We also wondered if we heard the dispatcher correctly that a person got stabbed in the cheek with a fork. At one point Stephanie bravely gave me her humerus (which is pretty funny) and Amir gave me his stethoscope and cuff so I could learn the proper way to take a blood pressure. Thankfully, Stephanie’s paresthesia lasted only a few minutes. At the nearby Oceania Fire Station we laughed with an Army veteran who has seen more than his fair share of tragedies, discussed the merits of Cheryl Crow as a History Channel commentator, and had a surprising conversation about the nutritional problems of hot dogs that made me worry that firefighters may someday eschew donuts. I saw camaraderie being built during the down times as well as during the calls. And, I talked with a squad member and former court official about the ones that were saved, the ones that got away, and an aging parent with dementia. I was reminded that all of us have to hold on to our victories, let go of our defeats, and understand that we’re in this together.
Dr. Aravich & us outside Sentara Virginia Beach General Hospital
Throughout the day I was humbled and inspired by consistent displays of commitment and professionalism, humanism and compassion, and collegiality and mutual support. I saw a successfully aged person with a rare and serious injury that causes significant pain in others but did not in her and wondered if it would steal her independence. I saw an isolated older woman and cancer survivor with depression and abdominal pain and hoped that her GI cancer was not coming back. I saw a frightened young mother fighting addiction and hoped that today will be the first day of the rest of her life. I saw an injured skateboarder who should have known about helmets. I saw a scared older person with breathlessness and fatigue and a family history of heart attack who should not have been cutting grass in the middle of a hot day. I saw the basic life support team immediately recognized the severity of this situation and calmly and effectively take precautions before the paramedic arrived. I saw the paramedic take an ECG in the truck and learned later that it showed the more severe type of heart attack called a STEMI (ST Elevation Myocardial Infarction). I saw the paramedic taking care of this person inside the moving and turning ambulance by, e.g., drawing blood, giving nitroglycerine, sending ECG telemetry to the ED, and offering words of encouragement. Finally, on the 4th of July I saw a crying spouse, caring neighbors, and engaged citizens volunteering to help others when almost everyone else was relaxing.
If, in the Jeffersonian tradition, the pursuit of happiness importantly involves pursuing the greater good, then the VBVRS is full of happy people. And, if people are not distinguished by doing what they have to do but are distinguished by doing what they don’t have to do, the VBVRS is full of very distinguished people. Thank you Stephanie, Amir and the VBVRS for allowing me to see the important volunteer work you do without charging patients. Lives do indeed need saving, both physically and emotionally. All of you saved lives today. Is there any greater compliment? Meantime, a few words about hot dogs: it is OK to bad-mouth hotdogs—but not on the 4th of July.
Dr. Paul Aravich is a behavioral neuroscientist and Professor of Pathology & Anatomy, Internal Medicine, and Physical Medicine and Rehabilitation at Eastern Virginia Medical School (EVMS). He is the former of the Virginia Brain Injury Council and its Ad Hoc Neurobehavioral Committee. He also chaired the Virginia Governor’s Public Guardian & Conservator Advisory Board and sits on the Boards of the Mary Buckley Foundation for brain injury survivors & their families; the I Need a Lighthouse Foundation for suicide awareness; and Alternatives, a nationally recognized youth empowerment organization. He won an AOA Glaser Distinguished Teacher Award. It is the highest award for medical education in the United States and Canada and is presented at the annual meeting of the Association of American Medical Colleges. He also won a Virginia State Council of Higher Education Outstanding Faculty Award, which is Virginia’s highest award for research, teaching and service.
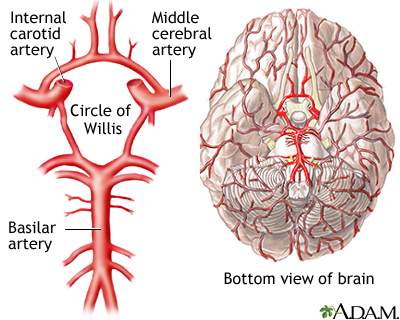
We all learned it in EMT-B class. The Cincinnati Prehospital Stroke Scale (CPSS) is the core assessment tool for EMS providers to evaluate possible stroke patients in the field. But, have you ever wondered where it came from? Why does it have 3 parts? Why test speech and not eyesight? What part of the brain is really injured? Let’s take a deeper dive.
What is the CPSS?
For a quick review, the CPSS is comprised of three individual tests, each of which get interpreted as either normal or abnormal by the EMS provider. The tests as well as interpretation are summarized in the table below.
Components of the Cincinnati Prehospital Stroke Scale
Adopted from Kothari, et al, 1996
Test
Normal
Abnormal
1
Facial Droop
Patient smiles or shows teeth
Both side of face move equally
One side of the face does not move as well as the other (or not at all)
2
Arm Drift
Patient extends arms out, closes eyes, and holds in place x 10 seconds
Both arms move the same, or both arms stay in position
One arm does not move or drifts downward compared to the other
3
Speech
Patient repeats “You can’t teach an old dog new tricks”
Patient repeats back correct words with no slurring of words
Patient can’t speak, says the wrong words, or slurs words
The CPSS is positive if any one of the three tests is deemed abnormal. In studies comparing Physicians vs EMS providers when performing the CPSS, when performed by an EMS provider, if the patient scored positive for one component, the sensitivity was 59%, meaning just over half of the patients who indeed had a stroke were identified by the EMS provider as having a stroke. The specificity was 89%, meaning that 89% of people who had a positive CPSS (1/3 components) indeed had a stroke. In other words, they caught just over half of the true strokes, but they also obtained a positive CPSS on some patients that didn’t have a stroke. The best example is a patient who is intoxicated. They likely have slurred speech, and therefore a positive CPSS, but aren’t actually having a stroke. Most tests in medicine are like this, you miss some, and you catch some that don’t really have the disease. We call these false negatives and false positives. Oh, and did I mentioned that EMT-Bs scored just as reliably as the Paramedics in the study?
The CPSS intentionally misses some strokes
To understand what the CPSS is looking for, it’s important to know a bit about the history of how it was created and why. The CPSS was developed at the University of Cincinnati Medical Center in 1997. tPA had just been approved by the FDA in June 1996. The CPSS is derived from the NIH Stroke Scale (NIHSS). You can read more about it here, but simply put, it’s a 15 part assessment where the patient gets scored according to their symptoms. The NIHSS was developed to identify neurological deficits that correspond to specific geographic tissue damage in the brain. MDCalc offers a great online calculator for helping determine a patient’s NIH Stroke Scale score. The NIHSS was condensed down, with some categories eliminated and some combined, to make the CPSS simple and easy to use, but also to help identify those patients who would be potential candidates for tPA. Not all strokes are created equal, and not all strokes are elligible for tPA, even if identified within the 4.5 hour time window. Strokes of the anterior cerebral artery and middle cerebral artery are better tPA candidates that other types of stroke. The CPSS focuses on identifying those strokes, but not posterior strokes for example.
The future of the CPSS and prehospital stroke identification
As I mentioned, the CPSS is not designed to detect things like posterior circulation strokes that affect the cerebellum, the balance center of the brain. Historically, efforts focused on early identification of tPA candidates. As new surgical and pharmacological advancements develop for other types of stroke, there’s a greater emphasis on early identification of all strokes. As such, there’s a lot of research going on right now studying new or modified prehospital stroke assessment tools. One front-runner is the B-FAST, which adds one more test to the CPSS to test for balance, and potentially identify posterior circulation strokes. The posterior circulation (basilar artery in the diagram above) supplies blood flow to the cerebellum, the balance center of the brain.
B– Balance, tested by having the patient walk
F– Face, same as CPSS
A – Arms, same as CPSS
S – Speech, same as CPSS
T – Time, to remind us that time is brain
If you want to impress with your turnover on your next stroke patient, be sure to test for balance disturbances by (carefully) ambulating your patient. If the patient stumbles or can’t walk without assistance, that’s a pertinent positive. In the original Cincinnati study by Kothari, the CPSS missed 13 patients with stroke, but 10 of those were posterior circulation strokes, notoriously difficult to diagnose clinically, and often missed by even the best Emergency Medicine physicians.
As always, feel free to share any tips you have on helping assess for stroke in the field.
~Steph
Some references:
Kothari R1, Hall K, Brott T, Broderick J. Early stroke recognition: developing an out-of-hospital NIH Stroke Scale. Acad Emerg Med. 1997 Oct;4(10):986-90.
Kothari RU1, Pancioli A, Liu T, Brott T, Broderick J. Ann Cincinnati Prehospital Stroke Scale: reproducibility and validity. Emerg Med. 1999 Apr;33(4):373-8.













































 Stephanie Krebs and Amir Louka are two
Stephanie Krebs and Amir Louka are two