I had a patient last week brought into the Pediatric ED for an allergic reaction. The child had known allergies, and by the EMR, had been prescribed an EpiPen by the Pediatrician – but mom said she didn’t have one at home to use. “We have insurance, but when I tried to fill the prescription, they wanted $620! I just can’t afford that,” she apologetically told me. I sat there in disbelief, assuming she had crappy insurance.
Flash forward three days later when the news hits the mainstream media:
AEMTs and Paramedics, better check that drug box twice for your 1:1000 epi vials because you’ll be using them more often for anaphylaxis as parents and patients increasingly forgo the EpiPen. With a $400-$650 price tag (with insurance), and a 1 year expiration date, can you blame them? I certainly don’t. So brush up on your local protocols, and stay vigilant. For a good review on anaphylaxis, check out this post.
Emergency Department (ED) Implications
As with prehospital providers, we too need to be ready with the IM epinephrine. It’s always been recommended after EpiPen administration for patients to come to the ED to be observed for 4-6 hours in case they need a redose of epinephrine. As patients increasingly skip that first dose, we should expect more potential for respiratory distress and need for difficult airway management.
EpiPen Alternative
Thanks to the Facebook Group EM Docs, I learned of AdrenaClick, a reasonable alternative we can prescribe for patients with severe allergies. The mechanism of delivery is slightly different than the EpiPen (two caps to remove instead of one), but given that it’s 1/4 the cost – it’s what I’ll be prescribing moving forward. AdrenaClick has a good training video on their website with detailed instructions for use. With a coupon from GoodRx, AdrenaClick is available for as low as $141.67 at Wal-Mart. It’s still more than the original $57 cost of an EpiPen when acquired by Mylan, but better than current EpiPen prices.
If you want to learn more about the skyrocketing prices of the EpiPen and the not-so-coincidental tie to congressional mandates requiring EpiPens (like AEDs) in schools, check out this article on Bloomberg.
<Disclaimer> And, of course, I do not endorse the efficacy of, nor am I paid by AdrenaClick. They just happen to be the only other comparable epi auto-injector on the market right now. <Disclaimer />
In April, 2016, Richmond became the first city in Virginia to partner with the CPR crowdsourcing app PulsePoint, bringing their technology to our city. Across the US the incidence of sudden cardiac arrest is over 300,000/year, and survival rates are generally less than 10%. Early CPR and defibrillation can triple that number. Other municipalities have had success with the technology, with early data showing it to be an effective way to get a bystander’s hands on the chest prior to the arrival of EMS units.
While neither Steph nor I have been alerted by the app yet, one of our interns has had it go off not once but twice in just three months. I spent a while picking his brain about it last night so we could share his experience.
Amir: Ok Mike, you were telling me a couple of weeks ago that your PulsePoint actually went off. Could you just explain to anyone who maybe hasn’t heard of PulsePoint exactly what it is and why you have it?
Mike: Sure, PulsePoint is an app that’s tied with the local EMS dispatch. Whenever there’s someone nearby who needs CPR, people with the app get a notification and can respond to help. Essentially trying to do for CPR what tinder has done for online dating.
Amir: Perfect. Except preferable not to wait for the other person to swipe right as they have only moments to live. Got it. So it’s on your phone, just monitoring the EMS dispatch, waiting for some unsuspecting person to drop – and that’s where your story starts. Lay it on me and the rest of the English speaking world.
Mike: When the alert went off I was enjoying my day off watching Game of Thrones. I had received one alert previously that I didn’t respond to (that one was while I was in the hospital), so I recognized the alert. It was a nearby address, and “CPR Needed,” no other information. I threw a shirt on (always don appropriate PPE first) and ran out the door. When I got there, I identified myself as a doctor (liability much?) and was let in. The victim in question didn’t actually require CPR; I did a jaw thrust to keep the airway open, and literally 45 seconds later an EMS crew made their way in. And from there, EMS basically was running the show.
Amir: Ok so most importantly, have you seen this season’s finale? It was amazing.
Mike: I can’t believe they killed off [insert character you’ve only just finally felt an emotional connection to]. So unexpected.
Amir: Speaking of killing off, back to this maybe-dying person. How did you even know where to go?
Mike: Pulse Point has a pretty clean interface. When the alert came up it has a Google Maps type street grid.
Amir: How far away was the spot?
Mike: Just a block or so, looking into it the app will typically alert a provider within 1/4 of a mile, depending on the agency.
Amir: So pants on, shirt on, out the door – leisurely stroll down the block? Or were you hoofing it?
Mike: I think I had a decent clip going. Not a full on sprint.
Amir: You live about 1/4 mile from us. If that app ever puts a pin on our house I expect you to transform into Usain Bolt.
But ok so you’re keeping it cool, it’s their emergency not yours after all, and you show up. What kind of place? Apartment? House?
Mike: House; one I had biked past many times around the neighborhood.
Amir: What’s the etiquette here? Politely knock on the door or charge in like Superman? I imagine the latter comes with the risk of being, you know, shot to death. But for all you know it’s an innocent baby dying in there, and you’re literally the only person who can save her, right?
Mike: Yeah, the thought crossed my mind. There’s definitely a can of worms to be opened here: how do Good Samaritan laws apply to physicians, was the correct address sent through the app, the list probably goes on. But I knocked and was let in, so cross at least one of those concerns off the list.
Amir: Did they ask who you were or how you knew what was going on or what you were doing there? I mean no uniform, badge – you’re Joe Schmo for all they know.
Mike: It was pretty hectic and everybody just seemed to accept that I was there to help. No other questions asked.
Amir: What did you find in there?
Mike: Respiratory distress, cause unknown. As somebody who doesn’t have a background in EMS, approaching this in the field is definitely a different thought process than undifferentiated respiratory distress rolling into the ED. Differential diagnosis isn’t too important when your treatment options are limited to what you bring with you, which in this case was nothing.
Amir: Great point. Something more docs should keep in mind when EMS rolls in with a hot mess. So not breathing, could be overdose but could also be massive head bleed, who knows? You don’t even have gloves. So you jaw thrust, trying to avoid any and all fluid leakage, and just hope the cavalry arrives soon. You weren’t up for mouth to mouth?
Mike: In retrospect, I did have my Red Cross pocket mask in the depths of my closet. Now it’s been moved to the shelf in my kitchen.
Amir: That’s a great tip. If you’re going to use this app and respond to god-knows what, be as prepared as possible. Maybe a little kit for the car and home with some basic stuff – gloves and a barrier mask.
Mike: But that does lead into another thing I’ve been considering about PulsePoint. The cavalry in this case was less than a minute away. From their website, PulsePoint costs over $10,000 to implement, and another $10k to $28k a year to maintain. So the agencies most likely to be able to afford an extra service like PulsePoint are also the agencies that are well funded, and most likely to have an EMS crew right around the corner.
Amir: Ah so you think maybe we need to see some pre/post implementation outcome data. I’d say if that guy had been in cardiac arrest though, those 45 seconds could make a significant difference.
Mike: Oh sure, it’s definitely a good idea. Especially considering that you don’t need to be a doctor to get the app. Anybody who’s BLS certified or better can join up. And unless there are some hidden costs involved, it’s still less expensive than a lot of the other “bells and whistles” that EMS agencies can add to their toolkit.
Amir: {{*cough* ACLS drugs *cough*}} Any other tips for potential heroes out there?
Mike: Just the usual things that I’m sure are second nature to EMS providers. Expect the unexpected, prepare for as much as you can, and the number one rule, first do no harm to yourself. “Survey the scene, don’t expose yourself to harm” doesn’t get drilled into us a ton as docs, but there’s a reason it’s the first step in BLS training.
Amir: Perfect. So to sum up:
Get Dressed.
Don’t show up empty handed.
Watch your back. And your front.
Have a good lawyer, just incase.
Mike: Couldn’t put it better myself.
Amir: I love it. Thanks for sharing the story. I can’t believe it’s gone off not once but TWICE for you. I’ll let you have the last word to your now adoring public.
Mike: Flarhgunnstow.
I had to look up that last word. Apparently it’s this:
If you know CPR and are willing to help someone whose life depends on it, go to PulsePoint.org and see if your city has partnered. If you don’t know CPR yet, the American Heart Association website can help you find a CPR course.
~Amir
Michael Billet, MD is now a PGY-2 in Emergency Medicine at VCU Medical Center in Richmond, VA. He attended the University of Virginia for both his undergraduate and medical school training. He likes long walks on the beach, Settlers of Catan, and is definitely the guy you want on your trivia team.
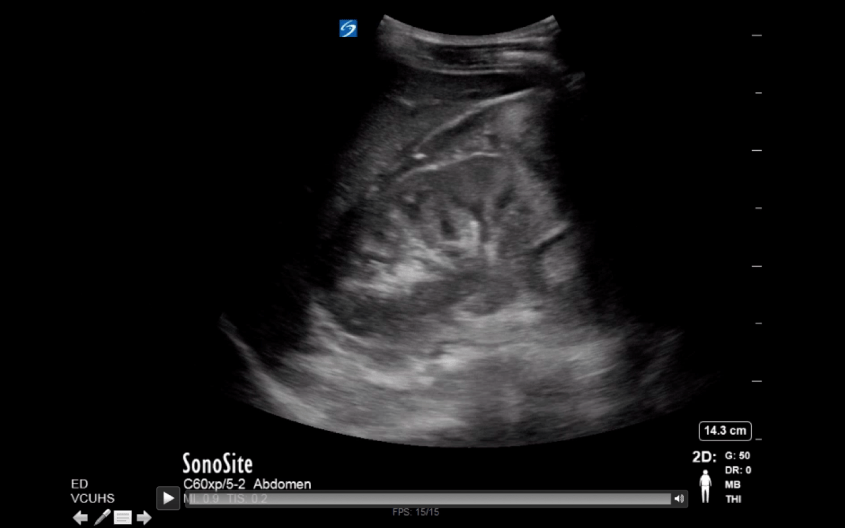
If you work in the medical field, you’ve likely had to present a patient case report. You do a chart review, gather the physical exam and lab data, but often importing the CT scans, ultrasounds, MRIs and other video imaging for display in your PowerPoint can be a time-consuming and frustrating task.
I recently discovered an easy way to include multimedia medical images into PowerPoint in a fairly easy way. This process works on a Mac. For PCs, I’ve been told Pacstacker is the best available option for importing radiology imaging into PowerPoint.
You’ll need access to 3 things to get started. Make sure you have each of these available on the same Mac:
The radiology image you want to capture, with the ability to scroll through
QuickTime includes a feature similar to the “Print Screen” feature. Instead of capturing just one image that instant, it captures your desktop activity in a selected area over time. The result is a video file you can import into PowerPoint or other presentation software.
Step 1: Open up your Radiology imaging viewer and select the scan you wish to include.
Step 2: Open QuickTime. From the File menu, select “New Screen Recording.”
Step 3: When the “Screen Recording” box pops up, click the red circular button to begin.
Step 4: A tan box will appear, asking you either click once to record the full screen, or drag and select with your mouse the portion of your screen you want included in your screen capture. For capturing radiology images, you’ll want to make sure you include only the image and exclude any personal identifiers to be HIPAA compliant.
Step 5: While recording, scroll through your imaging study making sure to include everything you want to display. I recommend scrolling through by clicking the arrows on the keyboard rather than using the mouse, as the cursor may accidentally enter the image field and therefore appear in your presentation.
Step 6: Click the “Stop” button to stop recording your screen capture. The button is somewhat hidden in the bar at the top of the screen. It’s the circular icon with the square in the middle that you see in the image below (right side of the screen, leftmost).
Step 7: After you click “Stop,” you’ll be prompted to save your video to your computer. Remember the location; you’ll need to find it later when you import your video into PowerPoint.
Step 8: Open your PowerPoint presentation. To import your imaging study, Go to Insert>Movie>Movie from File. Then find your file and click OK.
Step 9: Your imaging study is now imported into PowerPoint as a video. You can scroll backward and forward as needed during your presentation. To preview your video, start your presentation and click the triangular “Play” button on the bottom left. Note: if you click anywhere else on the slide, it will advance to your next slide, not start your video.
PowerPoint has improved over the years, and videos are now automatically embedded with your presentation when you save your .PPTx file. You may need to save your presentation file to DropBox, Google Drive or another cloud storage app as the file size is usually too large to send via email.
So that’s it – a previously arduous task made surprisingly simple. I hope this saves you some stress and time.
Apparently 12-1 is not an acceptable ratio when it comes to his & hers blogging… So in the interest of continued marital harmony, here’s a few thoughts to newbies on making yourself heard in the resus room.
It happens to the best of us. You’ve been sitting around the station all night and finally decide it’s safe to slip the boots off, only to be immediately reminded that the trauma gods do in fact enjoy tormenting you. On come the lights, quickly followed by a dispatcher’s pressured voice. As you glance at the clock reading 3am, a few words stand out. Gunshot wound. Bleeding. Unconscious.
For the next fifteen minutes you’re on autopilot – reflexively cutting away clothing, occluding that bubbling hole in the chest and dropping a needle down through the second intercostal space, just like you were trained. You watch the vital signs move back towards normal and you justifiably feel like a total badass. Time to load and go.
As you wheel into the trauma bay at your local Level 1, you’re confident you’ve done everything right. There’s the team, gowned and gloved, ready to take over.
“………..”
Inside your brain is screaming, “Work mouth, you bastard!” Now is the time to prove to all these doctors how awesome you are, how you saved this guy’s life. “I’ve done all the hard work. Speak damn you!”
“Ummm.. This is Steve, he’s a male..”
“SPEAK UP.”
“Steve! He’s a male! And.. we found him outside the bar – the one over off Main, well Main and 3rd… closer to 4th. He has asthma and…”
“Airway’s patent! Breath sounds clear bilaterally!” It’s too late. You lost them.
Want to keep the brief attention of your ED colleagues and trauma team? Here’s how:
1. Figure out who’s doing the talking – most critical patients roll in flanked by a entourage of medics, EMTs, fire fighters and/or police. Add to that the near-limitless helping hands in a large ED and there’s usually no need for the AIC to be occupied with distracting tasks like moving the patient off the stretcher or switching O2 from the portable tank to wall supply. Instead, the AIC should be at the foot of bed, addressing the entire room. Yes, everyone – the doctors, nurses, techs, social worker, chaplain and ogling med students ALL need to hear what’s going with this guy, so be ready to project your voice and speak clearly. And if you are the trainee, don’t disappear to clean the stretcher – stick around and listen. It’ll be your turn before you know it.
2. Take a deep breath – You made it. Even if the patient is actively coding, you’re here and your job is almost done. The blood splattered sidewalk, flashing lights, noise and confusion are all behind you. It’s our job to shut up and listen, and we will – for about 30 seconds. Starting your turnover in a calm and collected manner is the first sign to us those precious seconds will be well spent.
3. Age. Sex. Chief complaint/most pressing issue. – The first two always go off without a hitch. The third seems obvious, but every now and then it just takes an inexplicably long time to get around to mentioning the multiple stab wounds or EKG reading ***STEMI***STEMI***STEMI***. By the end of your first sentence we should know who your patient is and what went so wrong with their day to now be spending it with all these highly trained individuals.
4. Stay focused – This is not the time for an exhaustive presentation of the history and physical. A remote history of paronychia isn’t of much interest in someone with hemiparesis, but the time of onset certainly is. We can wait to hear she takes 500mg of Vitamin C daily, but Coumadin is a med I want to know about up front. By far this is the most difficult thing to master, because it often means reading our minds, knowing what’s important and what isn’t. A few stand out items in no particular order would be: loss of consciousness yes or no, symptoms improving or worsening, mechanism of injury, relevant surgeries, and medications including blood thinners, cardiac drugs such as beta blockers, and insulin.
5. Vitals – What are they now? Were they different at any time? What do you mean you only got one set?
6. Injuries, EKGs, physical exam and what did you do about it? – This is your chance to brag. “Patient was altered and EKG showed sinus bradycardia. I gave 0.5mg Atropine x1 with improvement in heart rate and mental status.” “The right leg was shortened with deformity at the mid-thigh. I gave 100mcg of Fentanyl and applied a traction splint.”
7. Access – ET tube, King airway, NPA? What size IVs and where are they? Did you drill IOs instead? Kudos if you did.
That’s it really. In 15-30 seconds we should hear what’s wrong with this person, how did it happen, what changes happened while he/she was with you and what did you do about it.
Giving a concise, accurate turnover takes practice. The pressure is on and your adrenaline is already up. You’re mentally exhausted, but those last few moments before he or she is off your stretcher are often the only insight doctors get into what’s going on, so make them count. Once the dust has settled, feel free to pull any of us aside for some feedback.
With that in mind, I realized that learning how to interact with the staff in the Emergency Department (ED) is also an art not often addressed in EMS education. Clearly you need to know and execute your protocols effectively – but how can you stand out as a respected EMS provider? Fortunately, I’ve been friends with an awesome charge nurse named Katie Arnold since junior high. She was kind enough to answer a few questions.
Steph: How long have you been a nurse, and how did you get to be a charge nurse?
Katie: I have been a nurse for 14 years this May 2015 – I have spent my whole career in the emergency department. I was selected for charge nurse by my manager, trained by another charge nurse and then started on my own around 2006-2007.
Steph: What do you like most about your job?
Katie: As an emergency nurse in general I love the unpredictable and unexpected. I tell new nurses, patients and their families all the time that it’s like a jigsaw puzzle: you get a piece here and a piece there but you don’t figure out the whole picture until all the pieces are in place. I love that I can have 5 patients all with the same chief complaint and each will be managed totally differently. As a charge nurse I love being a representative for the department, working with ancillary staff, patients, families, nurses, and EMS. I am there to control the flow of the department, to be a professional example for everyone and handle many administrative duties. It adds a whole other dimension to the role of nurse that allows further development of a holistic nurse.
Steph: Can you explain the goals and responsibilities of a charge nurse, in particular, ways you interact and work with EMS?
Katie: The duties are numerous and in depth. With EMS, we are the liaison between rescue and the ED. EMS providers are the eyes, ears and hands in the field; they are going to paint the picture the charge nurse needs to determine how each ambulance patient that arrives will affect the balance of the ED at every moment. You must appreciate their role in addition to the roles of the ED staff. Their resources are vastly different than the staff in the ED. I think staff nurses as well as some charge nurses lose sight of that fact.
Steph: What makes a good EMT in your mind?
Katie: A good EMT knows their role, provides an accurate concise report of what they are transporting to the ED. They demonstrate professionalism despite the stresses presented by the patient, the scene and the ED. A good EMT knows when to address concerns and when not to.
Steph: Do you have any pet peeves of EMS providers?
Katie: Lengthy reports of extraneous information and lack of recognition about valid concerns of the ED staff. One cannot expect the ED staff to appreciate EMS constraints but then not care about the concerns of the ED staff.
Steph: What can EMS providers do to make your life as a charge nurse easier?
Katie: As Charge Nurse, I have to decide what type of bed is appropriate for the patient based on the EMS report. Do they need a heart monitor, a psych bed or oxygen? Not all rooms are equipped with the same capabilities. A good report provides me with the information to make this decision. Helpful EMS providers also note when the ED is busy, and go the extra mile to be team players. Whether it’s cleaning a bed or hooking a patient up to the monitor, while not the job of the EMS provider, it helps the patient get care faster.
Steph: Which EMS providers impress you and why?
Katie: Those who are clear, concise, professional both in front of their patient and amongst colleagues on the EMS and ED side. Providers that are open to and understanding of constructive criticism.
Steph: Any tips for a brand new EMT?
Katie: I believe that when a new group of EMT’s are coming out they should have an initial interaction with a charge nurse or liaison at the ED to discuss these topics and allow for questions they may have to be asked prior to starting on the road. If that’s not done formally, then an individual EMT should feel free to introduce themselves to ED staff and seek feedback on reports.
Steph: And finally just for my own curiosity, what’s it like to be charge nurse on July 1 when the new Intern doctors start?
Katie: I love to teach and educate, so it does not bother me as it does others. ED Staff tend to become frustrated because each new class of Interns is unaware of how each ED operates with different patterns and order sets, goals and metrics. Some doctors are more receptive to that fact than others. It can drastically slow the flow of the ED and directly affect the care of the patients. New Interns are successful as long as they are willing to listen.
So there you have it, straight from the boss’s mouth. My advice, pick one thing to try and start there. Good patient reports are 90% of the game. Once you nail that, the rest falls into place.