Fred, our driver and nature guide, arrived to pick us up 10 minutes early at 5:50am. “Dis is terrible! We must go. Should have been on dee road at 5:30am – will heet so much traffeek!” he proclaimed with annoyance. Now, it’s Saturday morning and here he was claiming that traffic could be overwhelming but made more tolerable by a 30 minute head start. “Why’s there so much traffic on a Saturday morning?” I asked. He explained to me that one Saturday, each month, everyone in Rwanda participates in a day of service, typically cleaning up the streets. The event brings everyone outside at once, and often leads to increased pedestrian traffic in the roads.
We made excellent time, cutting the 3 hour drive east to Akagera National Park down to just 2.5 hours. Fred drives this route as many as 5 times a week and just took a group there yesterday. Established in 1934, the park is roughly 1200 miles of woodland, swamps, low mountains and savannah. The park used to be much larger, but was reduced in size by about 40% in 1994 after the Genocide. As refugees returned to Rwanda, the government took land from Akagera and gave it to the refugees for new settlements.
Our vehicle was a classic Toyota Landcruiser with a pop-up metal roof. It could have seated 6, but we enjoyed the extra space with just 4 of us (Frank stayed back in Kigali as he’s a touch under the weather). The drive out to Akagera was just what I had been missing. We’ve spent the entire week in the city and hadn’t yet explored the countryside. We passed by small but busy villages with people carrying giant yellow plastic water jugs 3 at a time, 300+ pounds of green bananas for the market, piles of sticks the size of a VW… all balanced on top of their heads or on the backs of bicycles.
Most houses are simple squares made of bricks or rocks and plastered in clay. Bright blue front doors seem to be in style. Children and little goats play in the front yards. Unfortunately the potholes in the gravel road doomed me to take only blurry photos as we sped by.
We entered the park just before 9:00am after picking up our picnic lunches for later in the day. It took less than 5 minutes for the animals to start introducing themselves. The entire day was filled with not just brief sightings, but appearances of multiple species at lengths long enough for close study. I can’t recap the whole day in words, so I’ll just let the pictures tell the story.
Giraffes on the savannahBaboons hanging out with the ImpalaStopping to stretch our legs on the savannahBasil, Jane and Dr. SudhaZebras, plus multiple other friends in the background
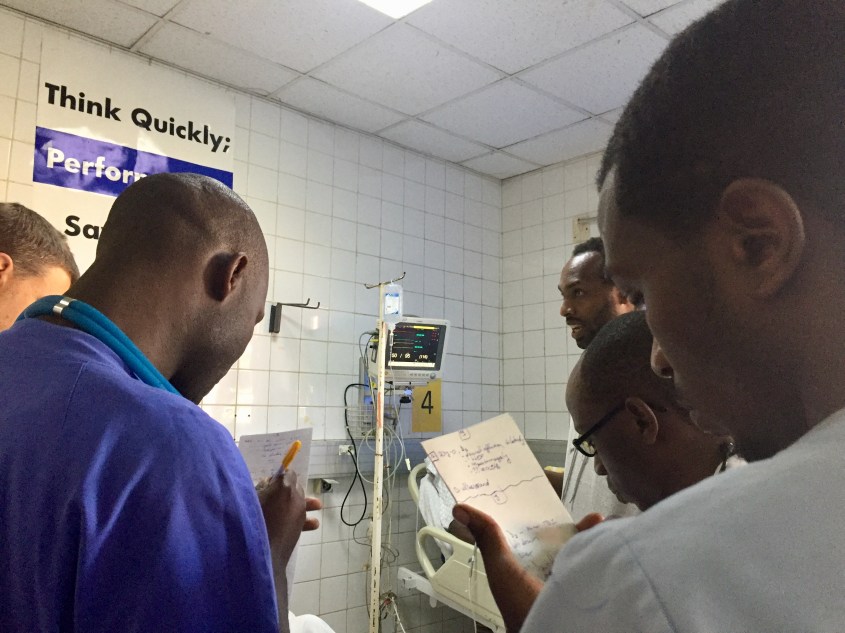
This morning Jane and I returned to Central University Hospital of Kigali (CHUK) to attend Rounds once again. Like Monday, we began in the RED Resuscitation room to see the most critical patients who arrived overnight.
In Bed 1 lay a man who initially went to a district hospital and had been transferred to CHUK just a few hours earlier. Previously healthy, about 3 weeks ago he began having fevers and then his whole body started to swell, which was followed shortly by trouble breathing. As soon as he arrived, the Emergency Medicine Resident performed a lung and heart ultrasound, and discovered fluid on both his lungs as well as a weak heart that didn’t squeeze as a heart of a man in his mid 30s should. I looked at the ventilator, and his oxygen reached only 85% at best. He’s likely suffering from a myocarditis. At home, this man would most likely be on ECMO, an advanced heart-lung bypass machine. Of course that’s not an option here, as ECMO isn’t even accessible in many places in the United States. His chances are slim if his oxygen levels do not improve.
Also in the RED room, we find a 10-week-old baby boy who suffered a severe TBI after a motorbike accident. Is it the same one my student was describing yesterday in class? The age is right, but this baby isn’t paralyzed. There must be two. Two 10-week-old babies with devastating neurological injuries after motorbike crashes. I can’t even imagine myself on one of these motorbikes nevertheless my infant daughter. I looked at the CT scan of the head and cringed – the skull was in 4 separate pieces, and somehow this baby was still alive.
The team rounding on YELLOW room patients
Over in the YELLOW room, I discovered the same man I met Monday, with the fractured femur, but with no money to pay for the operation to fix it. His doctors have been struggling all week to find him help, as they don’t want to send him home with a fracture that, without repair, will likely affect his ability to walk. I inquired about the cost of the surgery, remembering the suggestion of Dr. Noah that we all chip in to help him. Dr. Joe, today’s EM Attending, explained that bills for services are usually rolled up into a single line item, making understanding and predicting the cost of specific medications or procedures extremely difficult. Sounds just like the US. “If I had to guess, around $100,000 USD,” he says. There goes the dream of us funding his operation.
Triage is calm this morning
We shuffle as a group to the next bed, when overhead we hear, “CODE BLUE, Room 9 – CODE Blue Room 9.” We walk with purpose back towards the resuscitation room to discover a man with metastatic liver cancer who is unconscious and not breathing. The residents jump into action, bagging the man while they prepare for intubation and the potential for CPR. The man’s family is close by, and the Senior Resident takes a moment to discuss with them goals of care, as CPR and ventilator support will likely not help this man with terminal cancer. He uses words and phrases provided by Dr. Noah in his End of Life lecture from Monday. The man stabilizes with the respiratory support provided by the Resident, and we return to rounds, goals of care still unknown.
Families wait to pay their hospital bills. Discharges don’t happen until all debts are settled.
After Rounds, Jane and I walked back to our hotel, stopping to photograph some sights and for “African Tea” at the Camellia Tea House . It’s a mix of ginger tea and warm milk, sipped slowly and served with a butter cookie. Yum.
Jane has been on the hunt for some traditional Rwandan music to take back with her. We can’t seem to find CDs anywhere. I’m unsure if that’s because like back home, CDs are a dying format, or if we just haven’t stumbled upon the correct store.
A woman walks with a sack of something on her head
After shopping, we settled in for some lunch at our hotel. The food is good, but its appeal is more so the tropical balcony overlooking a busy intersection that lends itself to some excellent people watching. I’m cringing less each time as the motorbikes fly by, except when I see a baby on a mother’s back or a small child sandwiched between two adults on the same bike. There’s a stoplight at the intersection, but today it’s not in use. The convergence of cars, buses, motorbikes, pedestrians, cripples and cyclists is frenetic. I’m amazed there are no collisions. Back home in Richmond, our house too sits on the corner of an intersection, which despite much less traffic, has logged many more accidents and countless near misses.
Dr. Sudha arranged a lovely dinner at a restaurant with live music and traditional Rwandan dance to celebrate the conclusion of the courses for the week. Representatives from the Ministry of Health and Rotary joined us, as well as a few SAMU staff. Jane and I both wore African print dresses, because “When in Rome…,” right?
Tomorrow morning we are taking a safari tour to the Akagera National Park, just to the East, near the border with Tanzania. There’s potential to see leopards, lions, hippos, giraffes, zebras and more. We’re leaving at 6:00am to get there early before all the animals hide for the day.
Today was Day 2 of the Trauma Care Course. Things continued just as well as yesterday, so I don’t have too much to share. I gave two lectures, Musculoskeletal Trauma and Special Populations (Peds, OB, etc), then ran the students through the MCI/disaster table-top trainer. The students took their final exam, and based on the tests I graded vs the pretest, the improvements were remarkable. I can’t wait to see the statistical analysis of the score changes.
Memorable for me today was when one of my students asked me a “what would you have done?” question regarding a pediatric patient he had evaluated months ago. Motorbikes are common here as they are across Africa, and while there are helmet laws, there are still frequent, serious crashes. He responded to such a 912 call where 3 adults and a 10 week old baby were riding on a bike which crashed. Everyone but the baby had a helmet to protect the head. When he assessed the baby, he found it would not move its legs and indeed had a spinal cord injury causing paraplegia. He wanted to know how he could have stabilized the baby’s spine given that a cervical collar would not fit. I’m not sure I ever adequately answered his question because I couldn’t escape feeling a desperate hunger for a public health education program that might prevent such a crash entirely.
My favorite moment of the day was taking a photo with all of the inspiring women of SAMU. See, what’s interesting about Rwanda SAMU, is how many women they have on staff. I’m not sure if its because the staff all come from either nurse or nurse anesthetist background (both majority female) or something else, but a large portion are female. In the States, on average EMS is still male dominated since so many EMS systems are fire-based, and fire is disproportionately male. SAMU is third service (EMS separate from fire). I think these two things contribute to the number of amazing, unique women in the service.
I mentioned on Day 1 how captivated I was by the woman on the plane in the beautiful yellow dress. The clothing here is striking. Handmade dresses, blouses, wraps and jewelry in bright colors and patterns – Kigali rivals Europe in terms of fashion. I know I may be an independent feminist, but I also happen to believe fashion and feminism can coexist quite marvelously. Hence why I was desperate to take this picture with the inspiring, intelligent, gorgeous women of SAMU.
The women of Rwanda SAMU #WomeninEMS
Tomorrow the students begin a new educators’ course taught by Basil and Dr. Sudha to learn theories and best practices in adult education and EMS instruction. Monday and Tuesday next week they will then instruct the course they just completed today and propagate that knowledge to even more SAMU providers. I’m excited to hear how tomorrow’s course goes.
Jane and I will likely be at the hospital again for Rounds like Day 2. I say likely, because what I’ve quickly learned in Kigali, like many low and middle income countries, is that timelines and plans are fluid, and when things change (which they often do), you have to just go with the flow. So with that, I’ve set my alarm and will see where tomorrow takes me.
I knew it was going to be a good day when I went to take my shower this morning and discovered I had a washcloth. I’ve gotten it down to just two towels needed to mop up the floor. I’m learning.
Today marked the start of the Prehospital Trauma Care course we are here to teach. As I’ve mentioned in previous posts, we are here teaching a train-the-trainer type course to a select group of 25 students who will before we leave, teach the same content to an additional 25 students. Our goal is sustainability.
We opened the day with words of appreciation and encouragement from SAMU leadership as well as Frank and Ben, the Rotarians representing Williamsburg and Kigali chapters.
Basil created the course format to intermix thirty-minute lectures on major topics that were then each followed by simulation scenarios that put the concepts learned to the test. The students rotated roles as providers, patients, and evaluators. Those playing the role of family member did some Oscar-worthy acting, which seems to be a universal thing in EMS education. I’ve yet to run a scenario in an EMS course where there wasn’t Jerry Springer level on-scene drama.
Midway through the morning, we stopped for thirty minutes to “take tea” in the garden, which of course involved hot tea, but also samosas, cheese toast, coffee, and fresh juices. I think teatime needs to be implemented into all medical education programs as it was the perfect energy boost at just the right time.
Just before lunch, I reviewed major concepts in Airway & Breathing. The students, comprised of mostly Nurse Anesthetists and ED nurses, were up to date on the latest evidenced-based debates both for and against prehospital endotracheal intubation. The anesthetists did a show of hands for us to gauge how often they perform prehospital intubation. Counts ranged from 2 in the last 3 weeks to just 1 in 5 years. We discussed methods for achieving proficiency in an infrequently performed skill, the potential value of time saved with supraglottic airways, and avoidance of hypoxia as a way to improve outcomes. Despite not having fancy toys like video laryngoscopy, these guys know airway inside and out.
We ran the students through 4 unique scenarios, with major improvements made to communication, execution of primary and secondary surveys, and critical thinking. I don’t think there was a single scenario where we didn’t end up laughing at something. Hopefully the humor will help imprint some of these concepts for the students.
In the late afternoon, we practiced a variety of hands-on skills with designated simulation mannequins purchased with funds provided by the Rotary. Students experienced their first exposure to King airway, but also reviewed tried and true techniques such as needle decompression and insertion of oropharyngeal airways.
I think the jetlag and busy schedule are finally catching up with me. My goal is to be asleep by 10pm, so if I want to make it, I’d best wrap up writing for the night.
First on the agenda this morning after breakfast was a meeting with staff from the Ministry of Health to discuss the goals and vision for this partnership between VCU, Rwanda and Rotary International.
In April 1994, Rwanda experienced a 100 day genocide that resulted in 800,000-1,000,000 people killed, an estimated 20% of the country’s population. The genocide left the country economically and socially in tatters. It’s a complicated story, but well worth learning about if you are unfamiliar.
Rainshowers hover above Kigali
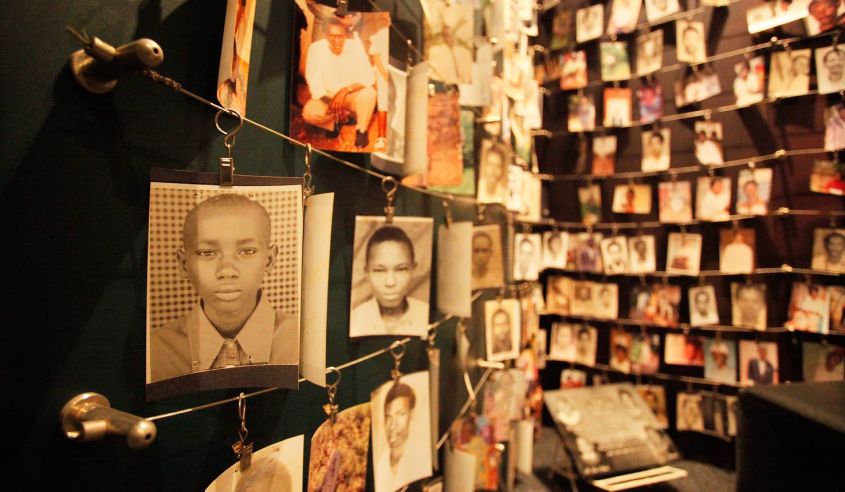
Next, we visited the Kigali Genocide Memorial. Our hosts were kind enough to escort us there and even provided us with flowers to place on the mass graves. I’m not even sure how to describe the experience, so I won’t try. But the museum is a sacred place, offering much to learn about humanity’s checkered past, and provides insight into how we can learn from all past genocide and work towards preventing any future conflicts.
Copyright: catnapsintransit.com
Incredibly, Rwanda has not only been able to heal from its history, but is on a track to reach middle-income status by 2020. President Kagame, who came to power after the genocide, established the Vision 2020 development program. He made healthcare one of the top priorities in his plan, the effects of which can be seen throughout the country.
A vision for a future Kigali, Copyright: archidatum.com
Per Wikipedia, “Rwanda has seen improvement on a number of key health indicators:
Between 2005 and 2013, life expectancy increased from 55.2 to 64.0,[310]
under-5 mortality decreased from 106.4 to 52.0 per 1,000 live births,[311]
incidence of tuberculosis has dropped from 101 to 69 per 100,000 people.”[312]
In our meeting, this focus was echoed. Working with SAMU, we are playing a small part in an overall strategy to improve healthcare by elevating and standardizing medical education, recording and analyzing data to assess patient outcomes and making evidence-based improvements to care. Rwanda is doing incredible things considering its resource limitations and is emerging as a thought-leader in healthcare delivery on the continent of Africa.
“Whoever saves a life, it is considered as if he saved an entire world.”
-Talmud
This was imprinted on glass at the Genocide Memorial. Today’s visit makes our work that much more meaningful. We are a part of the miracle of healing and rebuilding a nation and its people.
































")








")
")