

For 8 amazing summers, I worked as a lifeguard at Ocean Breeze Waterpark in Virginia Beach, VA. Some of the best memories in my life are from those days. However, unlike most lifeguard jobs – we actually saved drowning people, and A LOT of them, roughly 10-12 per day. I stopped counting my “saves” somewhere around 300. Looking back, this job was what lead me to EMS, and ultimately to becoming an Emergency Physician. The training provided by Ellis & Associates (E&A) created a great foundation of water rescue, first aid, CPR and leadership skills.

On a side note, you may be wondering how so many people can get into trouble at a water park. It’s not like the ocean, right? Well, I think as a society we have an inherent respect, and maybe some fear, of the ocean. Pools however, are clear and don’t have critters, so how dangerous can they be? People and parents let their guard down and get into trouble.
Are you a good lifeguard?
Before you read any further, I encourage you to take a little test. The two videos below both feature wave pools where there are active drowners. It’s like a high-stakes Where’s Waldo – can you spot the drowning victim? See if you could do the job.
Did you see the kids before the lifeguard blew the whistle to jump in? The kid in the first video has pretty obvious flailing; the kid in the second video – much more subtle. There’s been a great Slate.com article circulating around Facebook the last few months creating awareness that drowning doesn’t always look like what we expect.
Drowning Definitions
Before we get too deep into the medicine, let’s first talk terminology. Many of the terms I learned as a lifeguard have fallen out of favor in the medical community.
Drowning: a process resulting in primary respiratory impairment from submersion/immersion in a liquid medium
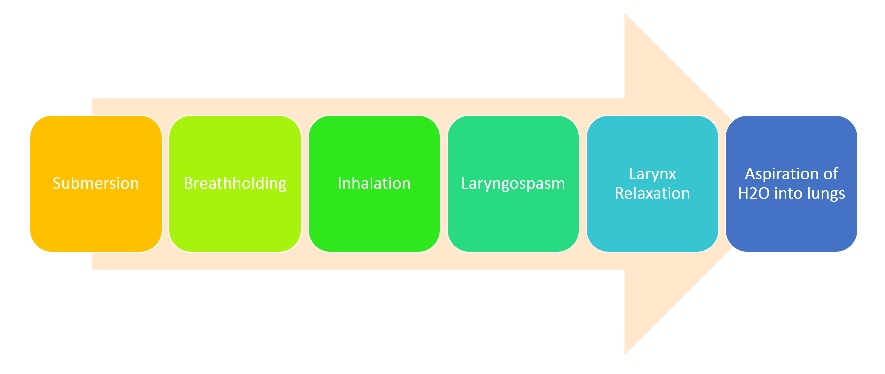
The Drowning Process: the period beginning with submersion into liquid, followed by breathholding. As oxygen is depleted and CO2 can’t be expired, the patient begins developing hypercarbia (high CO2), hypoxemia (low O2), and acidosis. As water is inhaled, the larynx spasms shut, blocking the exchange of air. As oxygen drops further, the laryngospasm relaxes, and the patient breathes water into the lungs. Recovery from the drowning process depends on when interventions are made and the resultant level of hypercarbia, hypoxemia, acidosis and encephalopathy.
Terms no longer used:
“Dry drowning” versus “wet drowning”: all drownings require some level of liquid, so they are all technically wet. What was traditionally called a “dry drowning” was just someone who made it to the laryngospasm step but no further because they left the water. “Wet drownings” went through a laryngospasm period, but advanced in the process to include inhalation of water into the lungs.
Managing Drowning Victims
You should of course follow your local protocols, but let’s talk about how the drowning mechanism affects care. Clearly if the victim has no pulse, you’ll follow ACLS/BLS guidelines and start CPR. If you get to a victim but can’t initiate chest compressions right away because you are oh I don’t know – in the middle of the ocean or a wave pool – at least try to give rescue breaths as you bring the victim to a more suitable place. Remember, drowning is primarily an airway issue, so any early airway interventions will be beneficial until you can start CPR. As of the 2010 AHA CPR updates, abdominal thrusts in a coding patient have been discarded for good old chest compressions. So, if your drowning victim isn’t breathing, even if they have a pulse you may need to do chest compressions for management of A&B.
Regarding when to intubate, per UptoDate, “in the symptomatic patient, indications for intubation include the following:
- Signs of neurologic deterioration or inability to protect the airway
- Inability to maintain a PaO2 above 60 mmHg or oxygen saturation (SpO2) above 90 percent despite high-flow supplemental oxygen
- PaCO2 above 50 mmHg” which is typically unavailable prehospital.
Whether someone was pulled from fresh or salt water is not particularly relevant to prehospital care as it doesn’t change management. Consensus used to be the patients in salt water were at risk for massive pulmonary edema and electrolyte imbalance in the blood as the high sodium content of the salt water shifted in the body. The risk and consequences of these shifts are now less worrisome than once thought. In a 150lb (70kg) person, it actually takes inhaling 5.5 cups of water before you’ll see osmotic water shifts in the body, and twice that before you’ll see electrolyte shifts.
The greatest risk of drowning of any type is hypoxemia leading to brain damage, and they key strategy is drowning prevention.
Drowning Prevention
Prevention is by far the best strategy in managing drowning, and in the last 20 years, smart safety measures and public education programs have helped drop the overall incidence of drowning by 9%, which includes a 45.6% drop for infants (< 1 yr of age). In fact, my good friend David Andrews who runs a water park out in California, told me that since the water park industry implemented a policy requiring kids <48″ to wear life jackets, active drowning events have declined roughly 50%.
So, if you are taking care of a drowning victim in your ambulance or ED, just follow your ACLS protocols. And, next time you are at the water park or pool, thank the lifeguard for their diligence and dedication, and please don’t complain that your kid has to wear a lifejacket.
~Steph











 level of anxiety to meet that of my patient won’t get anything done more quickly and certainly won’t hasten the cure.
level of anxiety to meet that of my patient won’t get anything done more quickly and certainly won’t hasten the cure.


