Today was Day 2 of the Trauma Care Course. Things continued just as well as yesterday, so I don’t have too much to share. I gave two lectures, Musculoskeletal Trauma and Special Populations (Peds, OB, etc), then ran the students through the MCI/disaster table-top trainer. The students took their final exam, and based on the tests I graded vs the pretest, the improvements were remarkable. I can’t wait to see the statistical analysis of the score changes.
Memorable for me today was when one of my students asked me a “what would you have done?” question regarding a pediatric patient he had evaluated months ago. Motorbikes are common here as they are across Africa, and while there are helmet laws, there are still frequent, serious crashes. He responded to such a 912 call where 3 adults and a 10 week old baby were riding on a bike which crashed. Everyone but the baby had a helmet to protect the head. When he assessed the baby, he found it would not move its legs and indeed had a spinal cord injury causing paraplegia. He wanted to know how he could have stabilized the baby’s spine given that a cervical collar would not fit. I’m not sure I ever adequately answered his question because I couldn’t escape feeling a desperate hunger for a public health education program that might prevent such a crash entirely.
My favorite moment of the day was taking a photo with all of the inspiring women of SAMU. See, what’s interesting about Rwanda SAMU, is how many women they have on staff. I’m not sure if its because the staff all come from either nurse or nurse anesthetist background (both majority female) or something else, but a large portion are female. In the States, on average EMS is still male dominated since so many EMS systems are fire-based, and fire is disproportionately male. SAMU is third service (EMS separate from fire). I think these two things contribute to the number of amazing, unique women in the service.
I mentioned on Day 1 how captivated I was by the woman on the plane in the beautiful yellow dress. The clothing here is striking. Handmade dresses, blouses, wraps and jewelry in bright colors and patterns – Kigali rivals Europe in terms of fashion. I know I may be an independent feminist, but I also happen to believe fashion and feminism can coexist quite marvelously. Hence why I was desperate to take this picture with the inspiring, intelligent, gorgeous women of SAMU.
The women of Rwanda SAMU #WomeninEMS
Tomorrow the students begin a new educators’ course taught by Basil and Dr. Sudha to learn theories and best practices in adult education and EMS instruction. Monday and Tuesday next week they will then instruct the course they just completed today and propagate that knowledge to even more SAMU providers. I’m excited to hear how tomorrow’s course goes.
Jane and I will likely be at the hospital again for Rounds like Day 2. I say likely, because what I’ve quickly learned in Kigali, like many low and middle income countries, is that timelines and plans are fluid, and when things change (which they often do), you have to just go with the flow. So with that, I’ve set my alarm and will see where tomorrow takes me.
I knew it was going to be a good day when I went to take my shower this morning and discovered I had a washcloth. I’ve gotten it down to just two towels needed to mop up the floor. I’m learning.
Today marked the start of the Prehospital Trauma Care course we are here to teach. As I’ve mentioned in previous posts, we are here teaching a train-the-trainer type course to a select group of 25 students who will before we leave, teach the same content to an additional 25 students. Our goal is sustainability.
We opened the day with words of appreciation and encouragement from SAMU leadership as well as Frank and Ben, the Rotarians representing Williamsburg and Kigali chapters.
Basil created the course format to intermix thirty-minute lectures on major topics that were then each followed by simulation scenarios that put the concepts learned to the test. The students rotated roles as providers, patients, and evaluators. Those playing the role of family member did some Oscar-worthy acting, which seems to be a universal thing in EMS education. I’ve yet to run a scenario in an EMS course where there wasn’t Jerry Springer level on-scene drama.
Midway through the morning, we stopped for thirty minutes to “take tea” in the garden, which of course involved hot tea, but also samosas, cheese toast, coffee, and fresh juices. I think teatime needs to be implemented into all medical education programs as it was the perfect energy boost at just the right time.
Just before lunch, I reviewed major concepts in Airway & Breathing. The students, comprised of mostly Nurse Anesthetists and ED nurses, were up to date on the latest evidenced-based debates both for and against prehospital endotracheal intubation. The anesthetists did a show of hands for us to gauge how often they perform prehospital intubation. Counts ranged from 2 in the last 3 weeks to just 1 in 5 years. We discussed methods for achieving proficiency in an infrequently performed skill, the potential value of time saved with supraglottic airways, and avoidance of hypoxia as a way to improve outcomes. Despite not having fancy toys like video laryngoscopy, these guys know airway inside and out.
We ran the students through 4 unique scenarios, with major improvements made to communication, execution of primary and secondary surveys, and critical thinking. I don’t think there was a single scenario where we didn’t end up laughing at something. Hopefully the humor will help imprint some of these concepts for the students.
In the late afternoon, we practiced a variety of hands-on skills with designated simulation mannequins purchased with funds provided by the Rotary. Students experienced their first exposure to King airway, but also reviewed tried and true techniques such as needle decompression and insertion of oropharyngeal airways.
I think the jetlag and busy schedule are finally catching up with me. My goal is to be asleep by 10pm, so if I want to make it, I’d best wrap up writing for the night.
First on the agenda this morning after breakfast was a meeting with staff from the Ministry of Health to discuss the goals and vision for this partnership between VCU, Rwanda and Rotary International.
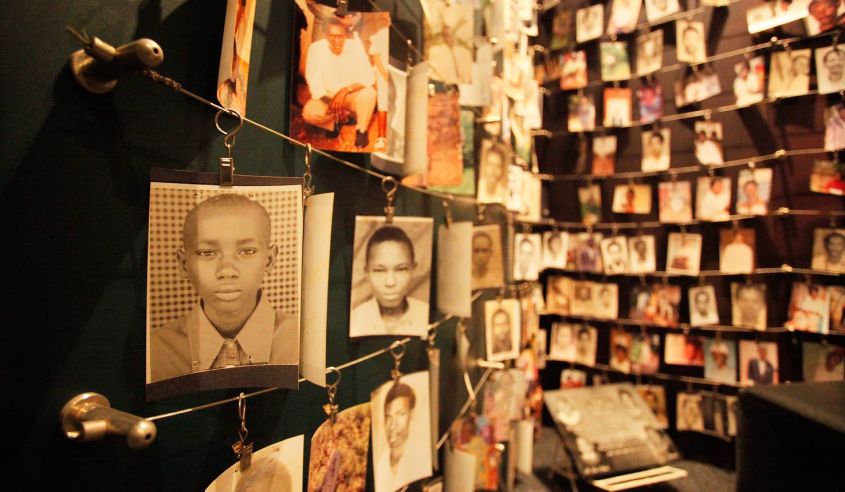
In April 1994, Rwanda experienced a 100 day genocide that resulted in 800,000-1,000,000 people killed, an estimated 20% of the country’s population. The genocide left the country economically and socially in tatters. It’s a complicated story, but well worth learning about if you are unfamiliar.
Rainshowers hover above Kigali
Next, we visited the Kigali Genocide Memorial. Our hosts were kind enough to escort us there and even provided us with flowers to place on the mass graves. I’m not even sure how to describe the experience, so I won’t try. But the museum is a sacred place, offering much to learn about humanity’s checkered past, and provides insight into how we can learn from all past genocide and work towards preventing any future conflicts.
Copyright: catnapsintransit.com
Incredibly, Rwanda has not only been able to heal from its history, but is on a track to reach middle-income status by 2020. President Kagame, who came to power after the genocide, established the Vision 2020 development program. He made healthcare one of the top priorities in his plan, the effects of which can be seen throughout the country.
A vision for a future Kigali, Copyright: archidatum.com
Per Wikipedia, “Rwanda has seen improvement on a number of key health indicators:
Between 2005 and 2013, life expectancy increased from 55.2 to 64.0,[310]
under-5 mortality decreased from 106.4 to 52.0 per 1,000 live births,[311]
incidence of tuberculosis has dropped from 101 to 69 per 100,000 people.”[312]
In our meeting, this focus was echoed. Working with SAMU, we are playing a small part in an overall strategy to improve healthcare by elevating and standardizing medical education, recording and analyzing data to assess patient outcomes and making evidence-based improvements to care. Rwanda is doing incredible things considering its resource limitations and is emerging as a thought-leader in healthcare delivery on the continent of Africa.
“Whoever saves a life, it is considered as if he saved an entire world.”
-Talmud
This was imprinted on glass at the Genocide Memorial. Today’s visit makes our work that much more meaningful. We are a part of the miracle of healing and rebuilding a nation and its people.
Traveler’s Rule: International travel will always be marked by adventures with foreign showers and toilets. This morning has already held true. Delighted to even have hot water, I prepped for my first shower. Dr. Sudha warned us yesterday, “There may or may not be a shower curtain, so make sure you put some towels on the floor to catch the water.” No problem, I thought.
It took 3 full-sized towels to mop up the lake on the floor. If I were wise, I would have toweled myself off and then cleaned the floor. Air-dry it is.
I woke up at 4:30am Kigali time (9:30pm EST) and couldn’t fall back asleep. For a second, I was startled by the mosquito net I’d wrapped myself in just a few hours earlier. I can get pretty claustrophobic at times. This might be one of them.
Breakfast is served each morning at our hotel, buffet style. As I’m writing and waiting to meet the team, I can hear the staff singing as they prepare the morning meal. I’m counting down the minutes until 6:00am when I get to experience my first cup of Rwandan coffee.
Breakfast did not disappoint. I’ll be eating fresh fruit and coffee for the rest of the trip each morning.
We walked up the hill from our hotel to the University Central Hospital of Kigali (CHUK) to join the team for 7:00am rounds on the patients in the Emergency Department. Dr. Noah, the ED Attending, is a US-trained Emergency Physician who is here for 7 years helping Rwanda reestablish its healthcare system.
After the genocide in 1994, many of the country’s doctors were either killed or fled the country secondary to the violence. That left a huge deficit in trained personnel that the country has been working to fill ever since. Grants have allowed many US physicians to come here and train the residents in an effort to rebuild. Rwanda opened its second medical school a few years after the genocide and plans to open a third in the near future. They have made amazing strides in a short time.
Dr. Noah facilitates a Resident discussion on end of life decisions and medical ethics
While I generally hate rounds (there’s a reason I chose Emergency Medicine), these were not your typical boring, Internal Medicine-type Rounds. The ED is organized into 4 large rooms, each with multiple beds with short curtains separating each.
The RED room is the resuscitation room for the sickest patients and contains 4 ventilators, one of which is currently out of service. I’m told the others are intermittently reliable. Resources are limited but they are providing excellent care with what they have. There we find multiple patients suffering from opportunistic infections, attributed to their HIV. There’s a YELLOW room with 6 beds. When RED patients improve, they are transitioned to this room. Here we found multiple patients suffering from trauma related mostly to the high rate of MVCs as I mentioned yesterday.
In bed 3, there’s a 38 year old man who was injured when a tree branch he was cutting fell on his neck, severing his spinal cord, resulting in quadriplegia. Rounds are conducted in English, but most of the patients we care for speak Kinyarwanda, Swahili or perhaps French. In a language I assume he doesn’t understand, we discuss his poor prognosis, as Rwanda has no long-term care facilities with spinal cord units, and motorized wheelchairs are a luxury available only to the super-wealthy.
He lays there on his back, with a cervical collar in place, staring at the ceiling and unable to make eye contact with us. We don’t speak to him, rather just about him, and I wonder if he understands his prognosis. I took a step forward, perhaps to make the interaction less cold, and realized he was crying. Although he’s stable right this moment, he’ll likely die in a week.
In room 3, the GREEN room, we meet a man who has suffered a femur fracture after a motorbike accident. He’s in the minority here as he has no insurance. Rwanda has a public insurance program where citizens pay minimal monthly fees, and if care is needed, the government pays 90% and the patient 10%. 5-10% of Rwandans choose not to participate, and unfortunately for this gentleman, he is in that minority. Unless in the case of true life threatening emergencies, labs and imaging are not ordered, medications withheld and surgeries postponed until the patients pay. Because of this, patients can spend days, weeks and in one case relayed to me, a month waiting to gather the required funds.
This man has no insurance and has no family or support system that could assist him with funding. He needs an orthopaedic surgery to install a metal plate to reattach the two ends of his femur. “Should we consider taking up a collection again?” offers Dr. Noah, and I realize this is a common challenge. We realize we aren’t going to solve this man’s problems quickly, and move on to the next bed to keep Rounds moving along.
After rounds we made our way just outside of the Emergency Department to Service d’aide médicale urgente (SAMU), the country’s ambulance service. Rwanda is 1/4 the landmass of Virginia, with a population nearly equivalent to that served by the Old Dominion EMS Alliance (ODEMSA), our regional EMS alliance for Central Virginia. SAMU staffs nurses and nurse anesthetists on the ambulance. Their training in prehospital medicine and trauma is minimal and variable, as there’s no standardized curriculum such as EMT and Paramedic. Most of the nurses and CRNAs worked in the ED prior to SAMU. The CRNAs can intubate and manage advanced medications, but the nurses cannot.
The ambulance bay contains a hodge-podge of ambulances – one way past its prime and slated for auction, another with random German writing which was donated, and another that could rival any newer model ambulance in the US. They utilize SUVs as smaller transport units, the backs of which look quite similar in setup to a medical helicopter. No CPR in these I’m afraid, but they look pretty darn cool and provide versatility in the crowded streets.
On the side of each ambulance is “Imbangukiragutabara,” meaning “Fast to Save.” We asked for help pronouncing it.
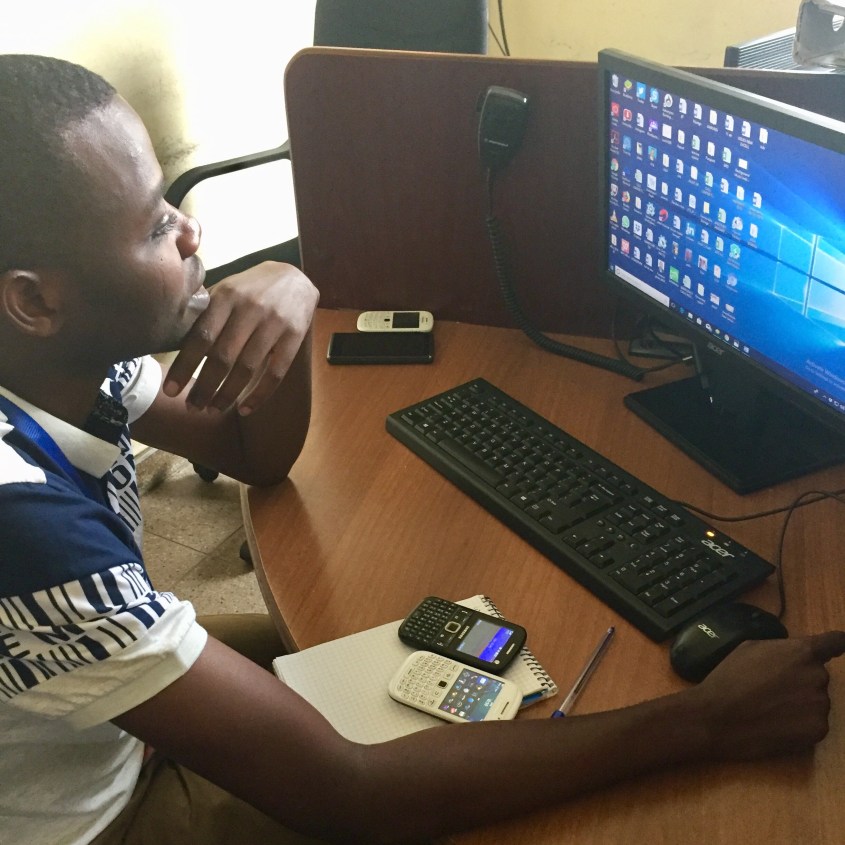
Because of their compact size, there’s really not room to ride along as an observer on the ambulance. I did however get to see the 912 (their 911) Dispatch Center that services the entire country. Calls come in from both landlines and cellular phones, but pinning down the exact location of the patient who needs care is challenging for many reasons:
Most houses don’t have numbers. Most callers are members of a citizen brigade of non-medical personnel who live out in all the villages and volunteer their time to help with emergencies. Fortunately these volunteers know their neighborhoods inside and out, and can take SAMU to the patients.
Cell phone calls don’t send the dispatcher any location data. In the US, we have federal regulations (Enhanced 911), mandating the data that cell phone carriers must provide to 911 centers. This doesn’t exist here.
Cell phone calls frequently disconnect. In the US, if this happens, the dispatcher can redial the initial number that called. Rwanda 912 will also try to call back, but if no one picks up, there is nothing they can do after that. In the US we often do location welfare checks if calls disconnect, but without early transmission of location data, this option disappears.
The 912 call center for Rwanda. Calls come into the white phone. Calls roll over to the black phone if the white phone is busy.
I had more to add for the day, but the WiFi has slowed to a crawl, and I need some sleep before tomorrow. Our day is packed with plans to visit the Ministry of Health, prepare the equipment for our course, and see the Genocide Museum.
~Steph
Oxygen tanks supplying the ORsAmbulances are well-stocked and organized
Coordinating the safe and timely travel of 2 physicians, 2 paramedics/RNs and 1 Rotarian from 2 different states and 3 different cities is no small undertaking. In addition to personnel, we had the added challenge of getting 300+ pounds worth of medical training equipment including CPR mannequins, needle decompression trainers and oxygen bottles to Rwanda with us. We found out about 4 weeks before we were to fly that these things aren’t readily available for purchase where we are headed.
We are going to Kigali, the capital of Rwanda, to teach. Our mission is to help build and solidify a formal EMS system with top-notch Prehospital trauma care. Ambulances in Kigali are currently operated by SAMU, but the providers are nurses rather than Paramedics or EMTs. That’s because there are no formal EMS certifications or programs there. Our aim is to provide the current workforce with prehospital-specific trauma training to improve provider safety. 50% of all EMS calls in Kigali are for motor vehicle collisions (MVCs). MVC trauma is a major cause of morbidity and mortality across Rwanda.
We carpooled from Richmond to Dulles. Basil, the creator of the Trauma Course content, was kind enough to offer up his Ford Explorer. More challenging than the traffic on I-95 though, were the back seat drivers offering our opinions on the best route. Dr. Sudha, a Trauma Surgeon and myself, an Emergency Physician – we are accustomed to being the pilots.
Fortunately the traffic gods showed us mercy, and we arrived at Dulles slightly ahead of schedule. The next challenge – get the 300+ lbs of luggage and equipment from the Explorer into the international terminal. It didn’t take long for the bellcap to notice me struggling to hoist a gigantic red backpack onto my back while desperately reaching for my rollerbag that was attempting to escape into traffic. He hurried towards us with his cart and began stacking our ridiculous assemblage of oversized bags. I can only imagine what he thought of us – between the bags marked “adult/child/infant” and “torso,” he must have thought we were body smugglers or really bad parents.
Inside the terminal, he unloaded our bags. I reached for some cash, knowing I was one of the few of us with smaller bills. In our pre-trip prep, Sudha advised us ahead of time to get $100 bills from the bank. In Rwanda, the larger the bill, the higher the exchange rate. I handed him the money and was met with a confused look. “Not enough, I said?” feeling confused and bordering on embarrassed. He mumbled something unintelligible but his face told me it wasn’t good. Frank, the Rotarian accompanying us on the trip, quickly slipped him more cash, which seemed to placate him as he then scurried away.
I have Dr. Sudha to thank for the opportunity to be on this trip. She’s a fellowship trained Trauma Surgeon with a focus on International Medicine. She and I have worked together for over three years in the Emergency Department at VCU taking care of trauma patients who suffer accidents and injuries throughout Central Virginia. She first travelled to Rwanda 7 years ago during her fellowship and has since made over 20 separate trips. (I get the sense she just stopped counting at some point). In October 2017, she was awarded 3 grants totaling over $700,000, one of which was from Rotary International; hence Frank’s presence with us on the trip. If you know her, you understand why she was trusted with so much money. She’s just impressive.
The 5th person travelling with us is Jane. A nurse and a volunteer paramedic in Deltaville, VA, Jane worked at VCU for years in multiple capacities. Over time, she’s carved out a niche in International EMS, so she was an obvious choice for the team.
Frank, Jane, Stephanie, Sudha and Basil
At the KLM* counter, we were met with friendliness and curiosity regarding our absurd quantity of baggage. We opted to check the medical equipment and carry-on our personal belongings. We didn’t want to take a gamble on the reliability of baggage transfer from Amsterdam to Kigali and end up with endotracheal tubes but no underwear.
I’ve decided for the privacy of those with me on the trip that I won’t include them from here on out. After all, this is just my perspective, and I don’t want to give the false appearance that I speak for anyone else. I will say I’m with a unique group of people and look forward to getting to know these like-minded folks. At dinner Dr. Sudha asked if we’d rather spend our 2 days off on a safari or at museums. The reflexive and immediate consensus was “SAFARI!” I knew then this was going to be a great trip.
*Bonus points for the free drinks on KLM.
Jan 21, 2018
“Day 2” is a bit of a misnomer. Technically it’s the 21st, but only because we just jumped ahead 6 hours by time zone. That didn’t stop KLM from feeding us breakfast just 1.5 hours after we’d eaten a full dinner.
We landed in Amsterdam without a hiccup. The last time I was in this airport was December of 2002. I’d just spent 5 months living in Spain, taking advanced conversational Spanish classes. What I didn’t realize then was just what a turn my life would take. I’d gone to Spain for a reset. I’d hit some professional hiccups in my last job and went to Spain, I thought, to do the study abroad I never had the chance to do while at UVA. Yes, I became fluent in Spanish, but I also found myself and my way forward.
What’s amazing about your twenties is the same thing that makes that time very lonely. You’ve left the nest, launched into a wide-open world full of opportunity, choices and possibilities. But you’ve left your nuclear family. And unlike decades prior, your independence isn’t quickly followed by love, marriage and establishment of your own nuclear family. There’s a gap now, a road with thousands of potential turns, each of which could lead to an entirely different life. Endless opportunity can be paralyzing. After standing at that airport, I came home, applied for and landed a job, which resulted in a successful career in Internet Marketing. I also joined my local rescue squad.
The view from the window on this leg of our journey, Amsterdam to Kigali, can be summed up in one word: tan. I finally gave in to my body’s repeated requests and took a 2 hour nap. Since waking up, I’ve seen nothing but desert. I did have a view of a beautiful part of Africa on the plane itself. Wearing a handmade, yellow and green gown with her hair secured tightly in a bright yellow wrap, everyone’s eyes focused on this woman when she appeared at the boarding gate. I looked down at my hold-over maternity pants and Merrill shoes and suddenly felt boorish and underdressed.
We arrived on time into Kigali. I had hoped for daylight as we landed so I could take an aerial survey of the city, but this close to the equator, night overcomes day very quickly, with sunsets happening in about 10 minutes from daylight to darkness.
We’re staying at the Gloria Hotel , which is just the right combination of nice but not stuffy. My only regret again is that it’s dark, and I can’t fully appreciate everything the area has to offer. I’m settling into my room as we have a long day tomorrow spending time in the Emergency Department, on the SAMU ambulance, and hopefully paying our respects at the Genocide Museum













")








")
")








")














")




